Tuberculous meningitis
Tuberculous meningitis, also known as TB meningitis or tubercular meningitis, is a specific type of bacterial meningitis caused by the Mycobacterium tuberculosis infection of the meninges—the system of membranes which envelop the central nervous system.[2][4]
| Tuberculous meningitis | |
|---|---|
| Other names | TB meningitis, Tubercular meningitis |
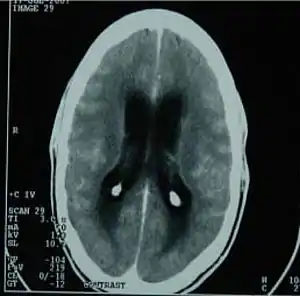 | |
| CT scan showing tuberculous meningitis | |
| Specialty | Neurology |
| Symptoms | Fever[1] |
| Causes | Mycobacterium tuberculosis[2] |
| Diagnostic method | Blood culture, CT scan[2] |
| Treatment | Antibiotic therapy and corticosteroids[3] |
Signs and symptoms
Fever and headache are the cardinal features; confusion is a late feature and coma bears a poor prognosis. Meningism is absent in a fifth of patients with TB meningitis. Patients may also have focal neurological deficits.[1][5]
Causes
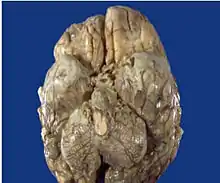
Mycobacterium tuberculosis of the meninges is the cardinal feature and the inflammation is concentrated towards the base of the brain.[6] When the inflammation is in the brain stem subarachnoid area, cranial nerve roots may be affected. The symptoms will mimic those of space-occupying lesions.[7]
Blood-borne spread certainly occurs, presumably by crossing the blood–brain barrier, but a proportion of patients may get TB meningitis from rupture of a cortical focus in the brain;[8] an even smaller proportion get it from rupture of a bony focus in the spine.[9]
Pathophysiology
The pathophysiology of tuberculous meningitis involves bacterial invasion of the brain parenchyma meninges or cortex, causing the formation of small subpial foci. These foci, termed Rich foci, are necrotic and expand as the colonies within them multiply. Tubercle (focal) rupture in the subarachnoid space causes meningitis.[3]
Diagnosis
Diagnosis of TB meningitis is made by analysing cerebrospinal fluid collected by lumbar puncture. When collecting CSF for suspected TB meningitis, a minimum of 1 ml of fluid should be taken (preferably 5 to 10 ml).[10] The CSF usually has a high protein, low glucose and a raised number of lymphocytes. Acid-fast bacilli are sometimes seen on a CSF smear, but more commonly, M. tuberculosis is grown in culture.[11] A spiderweb clot in the CSF that has been collected is rare but indicative of TB meningitis. ELISPOT testing is not useful for the diagnosis of acute TB meningitis and is often false negative,[12] but may paradoxically become positive after treatment has started, which helps to confirm the diagnosis.
Nucleic acid amplification tests (NAAT)
This is a group of tests that use polymerase chain reaction (PCR) to detect mycobacterial nucleic acid.[13] These test vary in which nucleic acid sequence they detect and vary in their accuracy. The two most common commercially available tests are the amplified mycobacterium tuberculosis direct test (MTD, Gen-Probe) and Amplicor.[14] In 2007, review concluded that for diagnosing tuberculous meningitis "Individually, the AMTD test appears to perform the best (sensitivity 74% and specificity 98%)", they found the pooled prevalence of TB meningitis to be 29%.[15]
Treatment
The treatment of TB meningitis is isoniazid, rifampicin, pyrazinamide and ethambutol for two months, followed by isoniazid and rifampicin alone for a further ten months.[16] Steroids help reduce the risk of death in those without HIV.[17] Steroids can be used in the first six weeks of treatment,[18] A few people may require immunomodulatory agents such as thalidomide.[19] Hydrocephalus occurs as a complication in about a third of people with TB meningitis. The addition of aspirin may reduce or delay mortality, possibly by reducing complications such as infarcts.[20][21]
References
- Harman, Robin J.; Mason, Pamela (2002-01-01). Handbook of Pharmacy Healthcare: Diseases and Patient Advice. Pharmaceutical Press. p. 93. ISBN 9780853695073.
- "Meningitis - tuberculous: MedlinePlus Medical Encyclopedia". www.nlm.nih.gov. Retrieved 2015-06-02.
- "Tuberculous Meningitis: Background, Pathophysiology, Etiology". 2018-05-23.
{{cite journal}}: Cite journal requires|journal=(help) - "Tuberculous Meningitis -- Medical Definition". www.medilexicon.com. Archived from the original on 2016-05-13. Retrieved 2015-06-02.
- Leach, Richard M. (2010-06-11). Acute and Critical Care Medicine at a Glance. John Wiley & Sons. p. 101. ISBN 9781444327229.
- Christodoulides, Myron (2013). Meningitis: Cellular and Molecular Basis. CABI. p. 154. ISBN 9781780641621.
- p1301 Robbins and Cotran, Pathologic Basis of Disease, 8th edition
- Nicoll, J. A. R.; Bone, Ian; Graham, David (2006-11-24). Adams & Graham's Introduction to Neuropathology 3Ed. CRC Press. p. 127. ISBN 9780340811979.
- Behera, D. (2010). Textbook of Pulmonary Medicine. Jaypee Brothers Publishers. p. 505. ISBN 9788184487497.
- "Cerebral spinal fluid (CSF) collection: MedlinePlus Medical Encyclopedia". www.nlm.nih.gov. Retrieved 2015-06-02.
- Irani, David N. (2008). Cerebrospinal Fluid in Clinical Practice. Elsevier Health Sciences. p. 196. ISBN 978-1416029083.
- Gram-Positive Bacterial Infections: Advances in Research and Treatment: 2011 Edition. ScholarlyEditions. 2012-01-09. p. 77. ISBN 9781464929717.
- Takahashi, Teruyuki; Tamura, Masato; Takasu, Toshiaki (2012). "The PCR-Based Diagnosis of Central Nervous System Tuberculosis: Up to Date". Tuberculosis Research and Treatment. 2012: 1–17. doi:10.1155/2012/831292. PMC 3359676. PMID 22666577.
- "CDC |TB | ...the Uses of Nucleic Acid Amplification Tests for the Diagnosis of TB: Background". www.cdc.gov. Retrieved 2015-06-02.
- Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, Drobniewski F, Lalvani A (2007). "A systematic review of rapid diagnostic tests for the detection of tuberculosis infection". Health Technol Assess. 11 (3): 1–196. doi:10.3310/hta11030. PMID 17266837.
- Barnett, Anthony H. (2006). Diabetes: Best Practice & Research Compendium. Elsevier Health Sciences. p. 146. ISBN 978-0323044011.
- Prasad, Kameshwar; Singh, Mamta B; Ryan, Hannah (28 April 2016). "Corticosteroids for managing tuberculous meningitis". Cochrane Database of Systematic Reviews. 2016 (4): CD002244. doi:10.1002/14651858.cd002244.pub4. PMC 4916936. PMID 27121755.
- Harrison, James; Kulkarni, Kunal; Baguneid, Mohamed; Prendergast, Bernard (2009). Oxford Handbook of Key Clinical Evidence. OUP Oxford. p. 336. ISBN 9780199234073.
- Central Nervous System Bacterial Infections—Advances in Research and Treatment: 2012 Edition: ScholarlyBrief. ScholarlyEditions. 2012-12-26. p. 28. ISBN 9781481616232.
- Rajshekhar, Vedantam (2009). "Management of hydrocephalus in patients with tuberculous meningitis Rajshekhar V Neurol India". Neurology India. 57 (4): 368–74. doi:10.4103/0028-3886.55572. PMID 19770534.
- Meningitis: New Insights for the Healthcare Professional: 2011 Edition: ScholarlyBrief. ScholarlyEditions. 2012-01-09. p. 2. ISBN 9781464905292.