Subunit vaccine
A subunit vaccine is a vaccine that contains purified parts of the pathogen that are antigenic, or necessary to elicit a protective immune response.[1][2] Subunit vaccine can be made from dissembled viral particles in cell culture or recombinant DNA expression,[3] in which case it is a recombinant subunit vaccine.
A "subunit" vaccine doesn't contain the whole pathogen, unlike live attenuated or inactivated vaccine, but contains only the antigenic parts such as proteins, polysaccharides[1][2] or peptides.[4] Because the vaccine doesn't contain "live" components of the pathogen, there is no risk of introducing the disease, and is safer and more stable than vaccines containing whole pathogens.[1] Other advantages include being well-established technology and being suitable for immunocompromised individuals.[2] Disadvantages include being relatively complex to manufacture compared to some vaccines, possibly requiring adjuvants and booster shots, and requiring time to examine which antigenic combinations may work best.[2]
The first recombinant subunit vaccine was produced in the mid-1980s to protect people from Hepatitis B. Other recombinant subunit vaccines licensed include Engerix-B (hepatitis B), Gardasil 9[5] (Human Papillomavirus), Flublok[6](influenza), Shingrix[7] (Herpes zoster) and Nuvaxovid[8] (Coronavirus disease 2019).
After injection, antigens trigger the production of antigen-specific antibodies, which are responsible for recognising and neutralising foreign substances. Basic components of recombinant subunit vaccines include recombinant subunits, adjuvants and carriers. Additionally, recombinant subunit vaccines are popular candidates for the development of vaccines against infectious diseases (e.g. tuberculosis,[9] dengue[10])
Recombinant subunit vaccines are considered to be safe for injection. The chances of adverse effects vary depending on the specific type of vaccine being administered. Minor side effects include injection site pain, fever, and fatigue, and serious adverse effects consist of anaphylaxis and potentially fatal allergic reaction. The contraindications are also vaccine-specific; they are generally not recommended for people with the previous history of anaphylaxis to any component of the vaccines. Advice from medical professionals should be sought before receiving any vaccination.
Discovery
The first certified subunit vaccine by clinical trials on humans is the hepatitis B vaccine, containing the surface antigens of the hepatitis B virus itself from infected patients and adjusted by newly developed technology aiming to enhance the vaccine safety and eliminate possible contamination through individuals plasma.[11]
Mechanism
Subunit vaccines contain fragments of the pathogen, such as protein or polysaccharide, whose combinations are carefully selected to induce a strong and effective immune response. Because the immune system interacts with the pathogen in a limited way, the risk of side effects is minimal.[2] An effective vaccine would elicit the immune response to the antigens and form immunological memory that allows quick recognition of the pathogens and quick response to future infections.[1]
A drawback is that the specific antigens used in a subunit vaccine may lack pathogen-associated molecular patterns which are common to a class of pathogen. These molecular structures may be used by immune cells for danger recognition, so without them, the immune response may be weaker. Another drawback is that the antigens do not infect cells, so the immune response to the subunit vaccines may only be antibody-mediated, not cell-mediated, and as a result, is weaker than those elicited by other types of vaccines. To increase immune response, adjuvants may be used with the subunit vaccines, or booster doses may be required.[2]
Types
| Types | Description | Examples |
|---|---|---|
| Protein subunit | contains isolated proteins from pathogens (virus or bacteria) | hepatitis B, acellular pertussis vaccines |
| Polysaccharide | contains chains of polysaccharides (sugar molecules) found in the pathogen's capsule such as cell walls of some bacteria | pneumococcal polysaccharide vaccine, meningococcal vaccine preventing diseases from Neisseria meningitidis group A, C, W-135, and Y |
| Conjugate | contains polysaccharide chains bound to carrier proteins, such as diphtheria and tetanus toxoid, to boost the immune response | pneumococcal conjugate vaccine, haemophilus influenzae type b conjugate vaccine, meningococcal conjugate vaccine |
Protein subunit
A protein subunit is a polypeptide chain or protein molecule that assembles (or "coassembles") with other protein molecules to form a protein complex.[12][13][14] Large assemblies of proteins such as viruses often use a small number of types of protein subunits as building blocks.[15] A key step in creating a recombinant protein vaccine is the identification and isolation of a protein subunit from the pathogen which is likely to trigger a strong and effective immune response, without including the parts of the virus or bacterium that enable the pathogen to reproduce. Parts of the protein shell or capsid of a virus are often suitable. The goal is for the protein subunit to prime the immune system response by mimicking the appearance but not the action of the pathogen.[16] Another protein-based approach involves self‐assembly of multiple protein subunits into a Virus-like particle (VLP) or nanoparticle. The purpose of increasing the vaccine's surface similarity to a whole virus particle (but not its ability to spread) is to trigger a stronger immune response.[17][16][18]
Protein subunit vaccines are generally made through protein production, manipulating the gene expression of an organism so that it expresses large amounts of a recombinant gene.[16][19] A variety of approaches can be used for development depending on the vaccine involved.[17] Yeast, baculovirus, or mammalian cell cultures can be used to produce large amounts of proteins in vitro.[16][19][20]
Protein-based vaccines are being used for hepatitis B and for human papillomavirus (HPV).[17][16] The approach is being used to try to develop vaccines for difficult-to-vaccinate-against viruses such as ebolavirus and HIV.[21] Protein-based vaccines for COVID-19 tend to target either its spike protein or its receptor binding domain.[17] As of 2021, the most researched vaccine platform for COVID-19 worldwide was reported to be recombinant protein subunit vaccines.[16][22]
Polysaccharide subunit
Vi capsular polysaccharide vaccine (ViCPS) against typhoid caused by the Typhi serotype of Salmonella enterica.[23] Instead of being a protein, the Vi antigen is a bacterial capsule polysacchide, made up of a long sugar chain linked to a lipid.[24] Capsular vaccines like ViCPS tend to be weak at eliciting immune responses in children. Making a conjugate vaccine by linking the polysacchide with a toxoid increases the efficacy.[25]
Conjugate vaccine
A conjugate vaccine is a type of vaccine which combines a weak antigen with a strong antigen as a carrier so that the immune system has a stronger response to the weak antigen.[26]
Peptide subunit
A peptide-based subunit vaccine employs a peptide instead of a full protein.[27] Peptide-based subunit vaccine mostly used due to many reasons,such as, it is easy and affordable for massive production. Adding to that, its greatest stability, purity and exposed composition.[28] Three steps occur leading to creation of peptide subunit vaccine;[29]
- Epitope recognition
- Epitope optimization
- Peptide immunity improvement
Features
When compared with conventional attenuated vaccines and inactivated vaccines, recombinant subunit vaccines have the following special characteristics:
- They contain clearly identified compositions which greatly reduces the possibility of presence of undesired materials within the vaccine.[30]
- Their pathogenicities are minimized as only fragments of the pathogen are present in the vaccine which cannot invade and multiply within the human body.[31]
- They have better safety profiles[32] and are suitable to be administered to immunocompromised patients.[33]
- They are suitable for mass production due to the use of recombinant technologies.[30]
- They have high stability so they can withstand environmental changes and are more convenient to be used in community settings.[31]
However, there are also some drawbacks regarding recombinant subunit vaccines:
- Addition of adjuvants is necessary during manufacturing to increase the efficacy of these vaccines.[34]
- Patients will have to receive booster doses to maintain long-term immunity.[34][35]
- Selection of appropriate cell lines for the cultivation of subunits is time-consuming because microbial proteins can be incompatible to certain expression systems.[35]
Pharmacology
Vaccination is a potent way to protect individuals against infectious diseases.[36]
Active immunity can be acquired artificially by vaccination as a result of the body's own defense mechanism being triggered by the exposure of a small, controlled amount of pathogenic substances to produce its own antibodies and memory cells without being infected by the real pathogen.[37]
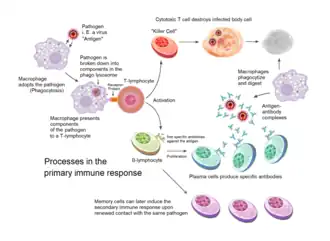
The processes involved in primary immune response are as follows:
- Pre-exposure to the antigens present in vaccines elicits a primary response. After injection, antigens will be ingested by antigen-presenting cells (APCs), such as dendritic cells and macrophages, via phagocytosis.[37][38]
- The APCs will travel to lymph nodes, where immature B cells and T cells are present.[39]
- Following antigen processes by APCs, antigens will bind to either MHC class I receptors or MHC class II receptors on the cell surface of the cells based on their compositional and structural features to form complexes.[37]
- Antigen presentation occurs, in which T cell receptors attach to the antigen-MHC complexes, initiating clonal expansion and differentiation, and hence the conversion of naive T cells to cytotoxic T cells (CD8+) or helper T cells (CD4+).[40][41]
- Cytotoxic CD8+ cells can directly destroy the infected cells containing the antigens that were presented to them by the APCs by releasing lytic molecules, while helper CD4+ cells are responsible for the secretion of cytokines that activates B cells and cytotoxic T cells.[38][42]
- B cells can undergo activation in the absence of T cells via the B cell receptor signalling pathway.[38]
- After dendritic cells capture the immunogen present in the vaccine, they can present the substances to naive B cells, causing the proliferation of plasma cells for antibody production.[43] Isotype switching can take place during B cell development for the formation of different antibodies, including IgG, IgE and IgA.[38]
- Memory B cells and T cells are formed post-infection.[37] The antigens are memorised by these cells so that subsequent exposure to the same type of antigens will stimulate a secondary response, in which a higher concentration of antibodies specific for the antigens are reproduced rapidly and efficiently in a short time for the elimination of the pathogen.[39]
Under specific circumstances, low doses of vaccines are given initially, followed by additional doses named booster doses. Boosters can effectively maintain the level of memory cells in the human body, hence extending a person's immunity.[34][35][44]
Manufacturing
The manufacturing process of recombinant subunit vaccines are as follows:
- Identification of immunogenic subunit
- Subunit expression and synthesis
- Extraction and purification
- Addition of adjuvants or incorporation to vectors
- Formulation and delivery.
Identification of immunogenic subunit
Candidate subunits will be selected primarily by their immunogenicity.[45] To be immunogenic, they should be of foreign nature and of sufficient complexity for the reaction between different components of the immune system and the candidates to occur.[46] Candidates are also selected based on size, nature of function (e.g. signalling) and cellular location (e.g. transmembrane).[45]
Subunit expression and synthesis
Upon identifying the target subunit and its encoding gene, the gene will be isolated and transferred to a second, non-pathogenic organism, and cultured for mass production.[47] The process is also known as heterologous expression.
A suitable expression system is selected based on the requirement of post-translational modifications, costs, ease of product extraction and production efficiency. Commonly used systems for both licensed and developing recombinant subunit vaccines include bacteria, yeast, mammalian cells, insect cells.[48]
Bacterial cells
Bacterial cells are widely used for cloning processes, genetic modification and small-scale productions.[49] Escherichia coli (E. Coli) is widely utilised due to its highly explored genetics, widely available genetic tools for gene expression, accurate profiling and its ability to grow in inexpensive media at high cell densities.[50]
E. Coli is mostly appropriate for structurally simple proteins owing to its inability to carry out post-translational modifications, lack of protein secretary system and the potential for producing inclusion bodies that require additional solubilisation.[49][50][51] Regarding application, E.Coli is being utilised as the expression system of the dengue vaccine.[10]
Yeast
Yeast matches bacterial cells' cost-effectiveness, efficiency and technical feasibility.[49] Moreover, yeast secretes soluble proteins and has the ability to perform post-translational modifications similar to mammalian cells.[51]

Notably, yeast incorporates more mannose molecules during N-glycosylation when compared with other eukaryotes,[52] which may trigger cellular conformational stress responses. Such responses may result in failure in reaching native protein conformation, implying potential reduction of serum half-life and immunogenicity.[49] Regarding application, both the hepatitis B virus surface antigen (HBsAg) and the virus-like particles (VLPs) of the major capsid protein L1 of human papillomavirus type 6, 11, 16, 18 are produced by Saccharomyces cerevisiae.
Mammalian cells
Mammalian cells are well known for their ability to perform therapeutically essential post-translational modifications and express properly folded, glycosylated and functionally active proteins.[50][53][54] However, efficacy of mammalian cells may be limited by epigenetic gene silencing and aggresome formation (recombinant protein aggregation).[50] For mammalian cells, synthesised proteins were reported to be secreted into chemically defined media, potentially simplifying protein extraction and purification.[49]
The most prominent example under this class is Chinese Hamster Ovary (CHO) cells utilised for the synthesis of recombinant varicella zoster virus surface glycoprotein (gE) antigen for SHINGRIX.[7] CHO cells are recognised for rapid growth and their ability to offer process versatility. They can also be cultured in suspension-adapted culture in protein-free medium, hence reducing risk of prion-induced contamination.[49][50]
Baculovirus (insect) cells
The baculovirus-insect cell expression system has the ability to express a variety of recombinant proteins at high levels and provide significant eukaryotic protein processing capabilities, including phosphorylation, glycosylation, myristoylation and palmitoylation.[55] Similar to mammalian cells, proteins expressed are mostly soluble, accurately folded, and biologically active.[56] However, it has slower growth rate and requires higher cost of growth medium than bacteria and yeast, and confers toxicological risks.[49] A notable feature is the existence of elements of control that allow for the expression of secreted and membrane-bound proteins in Baculovirus-insect cells.[49][55]
Licensed recombinant subunit vaccines that utilises baculovirus-insect cells include Cervarix (papillomavirus C-terminal truncated major capsid protein L1 types 16 and 18)[49][57] and Flublok Quadrivalent (hemagglutinin (HA) proteins from four strains of influenza viruses).[6]
Extraction and purification
Throughout history, extraction and purification methods have evolved from standard chromatographic methods to the utilisation of affinity tags.[58] However, the final extraction and purification process undertaken highly depends on the chosen expression system. Please refer to subunit expression and synthesis for more insights.
Addition of adjuvants
Adjuvants are materials added to improve immunogenicity of recombinant subunit vaccines.[59]
Adjuvants increase the magnitude of adaptive response to the vaccine and guide the activation of the most effective forms of immunity for each specific pathogen (e.g. increasing generation of T cell memory).[59][60][61][62] Addition of adjuvants may confer benefits including dose sparing and stabilisation of final vaccine formulation.[59][62]
Appropriate adjuvants are chosen based on safety, tolerance, compatibility of antigen and manufacturing considerations.[59] Commonly used adjuvants for recombinant subunit vaccines are Alum adjuvants (e.g. aluminium hydroxide), Emulsions (e.g. MF59) and Liposomes combined with immunostimulatory molecules (e.g. AS01B).[59][61]
Formulation and delivery
Delivery systems are primarily divided into polymer-based delivery systems (microspheres and liposomes) and live delivery systems (gram-positive bacteria, gram-negative bacteria and viruses)
Polymer-based delivery systems
Vaccine antigens are often encapsulated within microspheres or liposomes. Common microspheres made using Poly-lactic acid (PLA)[63] and poly-lactic-co-glycolic acid (PLGA)[63] allow for controlled antigen release by degrading in vivo while liposomes including multilamellar or unilamellar vesicles allow for prolonged release.[61]
Polymer-based delivery systems confer advantages such as increased resistance to degradation in GI tract, controlled antigen release, raised particle uptake by immune cells and enhanced ability to induce cytotoxic T cell responses.[61] An example of licensed recombinant vaccine utilising liposomal delivery is Shringrix.
Live delivery systems
Live delivery systems, also known as vectors, are cells modified with ligands or antigens to improve the immunogenicity of recombinant subunits via altering antigen presentation, biodistribution and trafficking.[64] Subunits may either be inserted within the carrier or genetically engineered to be expressed on the surface of the vectors for efficient presentation to the mucosal immune system.[47]
Advantages and disadvantages
Advantages
Disadvantages
- Reduced immunogenicity compared to attenuated vaccines[66][67]
- Can be difficult to isolate the specific antigen(s) which will invoke the necessary immune response[67]
- It is not easy to supervise conjugation chemistry which leads to noncontinuous variation[67]
Adverse effects and contraindications
Recombinant subunit vaccines are safe for administration.[68][69] However, mild local reactions, including induration and swelling of the injection site, along with fever, fatigue and headache may be encountered after vaccination.[68][70][71] Occurrence of severe hypersensitivity reactions and anaphylaxis is rare,[72] but can possibly lead to deaths of individuals. Adverse effects can vary among populations depending on their physical health condition, age, gender and genetic predisposition.[73][74]
Recombinant subunit vaccines are contraindicated to people who have experienced allergic reactions and anaphylaxis to antigens or other components of the vaccines previously.[75][76] Furthermore, precautions should be taken when administering vaccines to people who are in diseased state and during pregnancy,[75] in which their injections should be delayed until their conditions become stable and after childbirth respectively.
Licensed vaccines
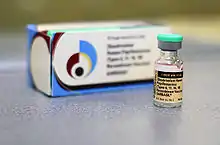
Hepatitis B
_vaccine.jpg.webp)
ENGERIX-B (produced by GSK) and RECOMBIVAX HB (produced by merck) are two recombinant subunit vaccines licensed for the protection against hepatitis B. Both contain HBsAg harvested and purified from Saccharomyces cerevisiae and are formulated as a suspension of the antigen adjuvanted with alum.[77][78]
Antibody concentration ≥10mIU/mL against HBsAg are recognized as conferring protection against hepatitis B infection.[77][78]
It has been shown that primary 3-dose vaccination of healthy individuals is associated with ≥90% seroprotection rates for ENGERIX-B, despite decreasing with older age. Lower seroprotection rates are also associated with presence of underlying chronic diseases and immunodeficiency. Yet, GSK HepB still has a clinically acceptable safety profile in all studied populations.[79]
Human Papillomavirus (HPV)
Cervarix, GARDASIL and GARDASIL9 are three recombinant subunit vaccines licensed for the protection against HPV infection. They differ in the strains which they protect the patients from as Cervarix confers protection against type 16 and 18,[57] Gardasil confers protection against type 6, 11, 16 and 18,[80] and Gardasil 9 confers protection against type 6, 11, 16, 18, 31, 33, 45, 52, 58[5] respectively. The vaccines contain purified VLP of the major capsid L1 protein produced by recombinant Saccharomyces cerevisiae.
It has been shown in a 2014 systematic quantitative review that the bivalent HPV vaccine (Cervarix) is associated with pain (OR 3.29; 95% CI: 3.00–3.60), swelling (OR 3.14; 95% CI: 2.79–3.53) and redness (OR 2.41; 95% CI: 2.17–2.68) being the most frequently reported adverse effects. For Gardasil, the most frequently reported events were pain (OR 2.88; 95% CI: 2.42–3.43) and swelling (OR 2.65; 95% CI: 2.0–3.44).[81]
Gardasil was discontinued in the U.S. on May 8, 2017, after the introduction of Gardasil 9[82] and Cervarix was also voluntarily withdrawn in the U.S. on August 8, 2016.[83]
Influenza
Flublok Quadrivalent is a licensed recombinant subunit vaccine for active immunisation against influenza. It contains HA proteins of four strains of influenza virus purified and extracted using the Baculovirus-insect expression system. The four viral strains are standardised annually according to United States Public Health Services (USPHS) requirements.[6]
Flublok Quadrivalent has a comparable safety profile to traditional trivalent and quadrivalent vaccine equivalents. Flublok is also associated with less local reactions (RR = 0.94, 95% CI 0.90–0.98, three RCTs, FEM, I2 = 0%, low‐ certainty evidence) and higher risk of chills (RR = 1.33, 95% CI 1.03–1.72, three RCTs, FEM, I2 = 14%, low‐certainty evidence).[84]
Herpes Zoster
SHINGRIX is a licensed recombinant subunit vaccine for protection against Herpes Zoster, whose risk of developing increases with decline of varicella zoster virus (VZV) specific immunity. The vaccine contains VZV gE antigen component extracted from CHO cells, which is to be reconstituted with adjuvant suspension AS01B.[7]
Systematic reviews and meta-analyses have been conducted on the efficacy, effectiveness and safety of SHINGRIX in immunocompromised 18-49 year old patients and healthy adults aged 50 and over. These studies reported humoral and cell-mediated immunity rate ranged between 65.4 and 96.2% and 50.0%-93.0% while efficacy in patients (18-49 yo) with haematological malignancies was estimated at 87.2% (95%CI, 44.3–98.6%) up to 13 months post-vaccination with an acceptable safety profile.[85][86]
COVID-19
NUVAXOVID is a recombinant subunit vaccine licensed for the prevention of SARS-CoV-2 infection. Market authorization was issued on 20 December 2021.[87] The vaccine contains the SARS-CoV-2 spike protein produced using the baculovirus expression system, which is eventually adjuvanted with the Matrix M adjuvant.[8]
History
While the practice of immunisation can be traced back to the 12th century, in which ancient Chinese at that time employed the technique of variolation to confer immunity to smallpox infection, the modern era of vaccination has a short history of around 200 years. It began with the invention of a vaccine by Edward Jenner in 1798 to eradicate smallpox by injecting relatively weaker cowpox virus into the human body.
The middle of the 20th century marked the golden age of vaccine science. Rapid technological advancements during this period of time enabled scientists to cultivate cell culture under controlled environments in laboratories,[88] subsequently giving rise to the production of vaccines against poliomyelitis, measles and various communicable diseases. Conjugated vaccines were also developed using immunologic markers including capsular polysaccharide and proteins.[88] Creation of products targeting common illnesses successfully lowered infection-related mortality and reduced public healthcare burden.
Emergence of genetic engineering techniques revolutionised the creation of vaccines. By the end of the 20th century, researchers had the ability to create recombinant vaccines apart from traditional whole-cell vaccine, for instance Hepatitis B vaccine, which uses the viral antigens to initiate immune responses.[88]
As the manufacturing methods continue to evolve, vaccines with more complex constitutions will inevitably be generated in the future to extend their therapeutic applications to both infectious and non-infectious diseases, in order to safeguard the health of more people.
Future directions
Recombinant subunit vaccines are used in development for tuberculosis,[9] dengue fever,[10] soil-transmitted helminths,[89] feline leukaemia[90] and COVID-19.[91]
Subunit vaccines are not only considered effective for SARS-COV-2, but also as candidates for evolving immunizations against malaria, tetanus, salmonella enterica, and other diseases.[11]
COVID-19
Research has been conducted to explore the possibility of developing a heterologous SARS-CoV receptor-binding domain (RBD) recombinant protein as a human vaccine against COVID-19. The theory is supported by evidence that convalescent serum from SARS-CoV patients have the ability to neutralise SARS-CoV-2 (corresponding virus for COVID-19) and that amino acid similarity between SARS-CoV and SARS-CoV-2 spike and RBD protein is high (82%).[91]
References
- "Module 2 - Subunit vaccines". WHO Vaccine Safety Basics e-learning course. Archived from the original on 2021-08-08.
- "What are protein subunit vaccines and how could they be used against COVID-19?". GAVI. Archived from the original on 2021-08-17.
- Francis MJ (March 2018). "Recent Advances in Vaccine Technologies". The Veterinary Clinics of North America. Small Animal Practice. Vaccines and Immunology. 48 (2): 231–241. doi:10.1016/j.cvsm.2017.10.002. PMC 7132473. PMID 29217317.
- Lidder P, Sonnino A (2012). "Biotechnologies for the management of genetic resources for food and agriculture". Advances in Genetics. Elsevier. 78: 1–167. doi:10.1016/B978-0-12-394394-1.00001-8. ISBN 9780123943941. PMID 22980921.
- "Gardasil 9 (Human Papillomavirus 9-valent Vaccine, Recombinant)". Food and Drug Administration.
- "Flublok Quadrivalent (Influenza Vaccine)". Food and Drug Administration.
- "Shingrix (Zoster Vaccine Recombinant, Adjuvanted)". Food and Drug Administration.
- "Nuvaxovid dispersion for injection,COVID-19 Vaccine (recombinant, adjuvanted)" (PDF).
- Mascola JR, Fauci AS (February 2020). "Novel vaccine technologies for the 21st century". Nature Reviews. Immunology. 20 (2): 87–88. doi:10.1038/s41577-019-0243-3. PMC 7222935. PMID 31712767.
- Tripathi NK, Shrivastava A (2018-08-23). "Recent Developments in Recombinant Protein-Based Dengue Vaccines". Frontiers in Immunology. 9: 1919. doi:10.3389/fimmu.2018.01919. PMC 6115509. PMID 30190720.
- Cuffari B (2022). "What is a Subunit Vaccine?". News medical lifesciences.
- Alberts B, Johnson A, Lewis J, Raff M, Roberts K, Walter P (2002). The Shape and Structure of Proteins. New York: Garland Science. Retrieved 15 April 2022.
- Stoker HS (1 January 2015). General, Organic, and Biological Chemistry (7th ed.). Boston, MA: Cengage Learning. pp. 709–710. ISBN 978-1-305-68618-2. Retrieved 15 April 2022.
- Smith MB (27 April 2020). Biochemistry: An Organic Chemistry Approach. Boca Raton: CRC Press. p. 269-270. ISBN 978-1-351-25807-4. Retrieved 15 April 2022.
- Vijayan M, Yathindra N, Kolaskar AS (1999). "Multi-protein assemblies with point group symmetry". In Vijayan M, Yathindra N, Kolaskar AS (eds.). Perspectives in Structural Biology: A Volume in Honour of G.N. Ramachandran. Hyderabad, India: Universities Press. pp. 449–466. ISBN 978-81-7371-254-8. Retrieved 15 April 2022.
- Plummer EM, Manchester M (2011). "Viral nanoparticles and virus-like particles: platforms for contemporary vaccine design". Wiley Interdisciplinary Reviews. Nanomedicine and Nanobiotechnology. 3 (2): 174–196. doi:10.1002/wnan.119. PMC 7169818. PMID 20872839.
- Hotez PJ, Bottazzi ME (January 2022). "Whole Inactivated Virus and Protein-Based COVID-19 Vaccines". Annual Review of Medicine. 73 (1): 55–64. doi:10.1146/annurev-med-042420-113212. PMID 34637324. S2CID 238747462.
- Noad R, Roy P (September 2003). "Virus-like particles as immunogens". Trends in Microbiology. 11 (9): 438–444. doi:10.1016/S0966-842X(03)00208-7. PMID 13678860.
- Wang M, Jiang S, Wang Y (April 2016). "Recent advances in the production of recombinant subunit vaccines in Pichia pastoris". Bioengineered. 7 (3): 155–165. doi:10.1080/21655979.2016.1191707. PMC 4927204. PMID 27246656.
- Bill RM (March 2015). "Recombinant protein subunit vaccine synthesis in microbes: a role for yeast?". The Journal of Pharmacy and Pharmacology. 67 (3): 319–328. doi:10.1111/jphp.12353. PMID 25556638. S2CID 22339760.
- Decker JM. "Vaccines". Immunology Course 419. Department of Veterinary Science & Microbiology at The University of Arizona. Archived from the original on 2003-06-10.
- Bayani F, Hashkavaei NS, Arjmand S, Rezaei S, Uskoković V, Alijanianzadeh M, et al. (March 2023). "An overview of the vaccine platforms to combat COVID-19 with a focus on the subunit vaccines". Progress in Biophysics and Molecular Biology. 178: 32–49. doi:10.1016/j.pbiomolbio.2023.02.004. PMC 9938630. PMID 36801471.
- Raffatellu M, Chessa D, Wilson RP, Dusold R, Rubino S, Bäumler AJ (June 2005). "The Vi capsular antigen of Salmonella enterica serotype Typhi reduces Toll-like receptor-dependent interleukin-8 expression in the intestinal mucosa". Infection and Immunity. 73 (6): 3367–3374. doi:10.1128/IAI.73.6.3367-3374.2005. PMC 1111811. PMID 15908363.
- Hu X, Chen Z, Xiong K, Wang J, Rao X, Cong Y (August 2017). "Vi capsular polysaccharide: Synthesis, virulence, and application". Critical Reviews in Microbiology. 43 (4): 440–452. doi:10.1080/1040841X.2016.1249335. PMID 27869515. S2CID 205694206.
- Lin FY, Ho VA, Khiem HB, Trach DD, Bay PV, Thanh TC, et al. (April 2001). "The efficacy of a Salmonella typhi Vi conjugate vaccine in two-to-five-year-old children". The New England Journal of Medicine. 344 (17): 1263–1269. doi:10.1056/nejm200104263441701. PMID 11320385.
- Pollard A. "Types of vaccine". Oxford vaccine group 2020. University of Oxford.
- Malonis RJ, Lai JR, Vergnolle O (March 2020). "Peptide-Based Vaccines: Current Progress and Future Challenges". Chemical Reviews. 120 (6): 3210–3229. doi:10.1021/acs.chemrev.9b00472. PMC 7094793. PMID 31804810.
- Skwarczynski M, Toth I (May 2011). "Peptide-based subunit nanovaccines". Current Drug Delivery. 8 (3): 282–289. doi:10.2174/156720111795256192. PMID 21291373.
- Kalita P, Tripathi T (May 2022). "Methodological advances in the design of peptide-based vaccines". Drug Discovery Today. Elsevier. 27 (5): 1367–1380. doi:10.1016/j.drudis.2022.03.004. PMID 35278703. S2CID 247399368.
- Soltanmohammadi B, Jalali-Javaran M, Rajabi-Memari H, Mohebodini M (February 2014). "Cloning, Transformation and Expression of Proinsulin Gene in Tomato (Lycopersicum esculentum Mill.)". Jundishapur Journal of Natural Pharmaceutical Products. 9 (1): 9–15. doi:10.17795/jjnpp-7779. PMC 3957137. PMID 24644433.
- Baxter D (December 2007). "Active and passive immunity, vaccine types, excipients and licensing". Occupational Medicine. 57 (8): 552–556. doi:10.1093/occmed/kqm110. PMID 18045976.
- Nascimento IP, Leite LC (December 2012). "Recombinant vaccines and the development of new vaccine strategies". Brazilian Journal of Medical and Biological Research. 45 (12): 1102–1111. doi:10.1590/S0100-879X2012007500142. PMC 3854212. PMID 22948379.
- Wang M, Jiang S, Wang Y (April 2016). "Recent advances in the production of recombinant subunit vaccines in Pichia pastoris". Bioengineered. 7 (3): 155–165. doi:10.1080/21655979.2016.1191707. PMC 4927204. PMID 27246656.
- Sedova ES, Shcherbinin DN, Migunov AI, Smirnov I, Logunov DI, Shmarov MM, et al. (October 2012). "Recombinant influenza vaccines". Acta Naturae. 4 (4): 17–27. doi:10.32607/20758251-2012-4-4-17-27. PMC 3548171. PMID 23346377.
- Andersson C. Production and delivery of recombinant subunit vaccines. OCLC 1301470908.
- Rodrigues CM, Plotkin SA (2020-07-14). "Impact of Vaccines; Health, Economic and Social Perspectives". Frontiers in Microbiology. 11: 1526. doi:10.3389/fmicb.2020.01526. PMC 7371956. PMID 32760367.
- Clem AS (January 2011). "Fundamentals of vaccine immunology". Journal of Global Infectious Diseases. 3 (1): 73–78. doi:10.4103/0974-777X.77299. PMC 3068582. PMID 21572612.
- Saylor K, Gillam F, Lohneis T, Zhang C (24 February 2020). "Designs of Antigen Structure and Composition for Improved Protein-Based Vaccine Efficacy". Frontiers in Immunology. 11 (283): 283. doi:10.3389/fimmu.2020.00283. PMC 7050619. PMID 32153587.
- LeBien TW, Tedder TF (September 2008). "B lymphocytes: how they develop and function". Blood. 112 (5): 1570–1580. doi:10.1182/blood-2008-02-078071. PMC 2518873. PMID 18725575.
- Kallon S, Samir S, Goonetilleke N (April 2021). "Vaccines: Underlying Principles of Design and Testing". Clinical Pharmacology and Therapeutics. 109 (4): 987–999. doi:10.1002/cpt.2207. PMC 8048882. PMID 33705574.
- Curtsinger JM, Johnson CM, Mescher MF (November 2003). "CD8 T cell clonal expansion and development of effector function require prolonged exposure to antigen, costimulation, and signal 3 cytokine". Journal of Immunology. 171 (10): 5165–5171. doi:10.4049/jimmunol.171.10.5165. PMID 14607916. S2CID 24326081.
- Klarquist J, Cross EW, Thompson SB, Willett B, Aldridge DL, Caffrey-Carr AK, et al. (August 2021). "B cells promote CD8 T cell primary and memory responses to subunit vaccines". Cell Reports. 36 (8): 109591. doi:10.1016/j.celrep.2021.109591. PMC 8456706. PMID 34433030.
- Wykes M, MacPherson G (May 2000). "Dendritic cell-B-cell interaction: dendritic cells provide B cells with CD40-independent proliferation signals and CD40-dependent survival signals". Immunology. 100 (1): 1–3. doi:10.1046/j.1365-2567.2000.00044.x. PMC 2326988. PMID 10809952.
- Meng H, Mao J, Ye Q (June 2022). "Booster vaccination strategy: Necessity, immunization objectives, immunization strategy, and safety". Journal of Medical Virology. 94 (6): 2369–2375. doi:10.1002/jmv.27590. PMID 35028946. S2CID 245933504.
- Lindskog M, Rockberg J, Uhlén M, Sterky F (May 2005). "Selection of protein epitopes for antibody production". BioTechniques. 38 (5): 723–727. doi:10.2144/05385ST02. PMID 15945371.
- Tijssen P, ed. (1985-01-01). "Chapter 4 The nature of immunogens, antigens, and haptens". Laboratory Techniques in Biochemistry and Molecular Biology. Practice and Theory of Enzyme Immunoassays. Vol. 15. Elsevier. pp. 39–41. doi:10.1016/S0075-7535(08)70134-7. ISBN 9780444806345.
- Liljeqvist S, Ståhl S (July 1999). "Production of recombinant subunit vaccines: protein immunogens, live delivery systems and nucleic acid vaccines". Journal of Biotechnology. 73 (1): 1–33. doi:10.1016/s0168-1656(99)00107-8. PMID 10483112.
- Francis MJ (March 2018). "Recent Advances in Vaccine Technologies". The Veterinary Clinics of North America. Small Animal Practice. 48 (2): 231–241. doi:10.1016/j.cvsm.2017.10.002. PMC 7132473. PMID 29217317.
- Ferrer-Miralles N, Domingo-Espín J, Corchero JL, Vázquez E, Villaverde A (March 2009). "Microbial factories for recombinant pharmaceuticals". Microbial Cell Factories. 8 (1): 17. doi:10.1186/1475-2859-8-17. PMC 2669800. PMID 19317892.
- Corchero JL, Gasser B, Resina D, Smith W, Parrilli E, Vázquez F, et al. (2013). "Unconventional microbial systems for the cost-efficient production of high-quality protein therapeutics". Biotechnology Advances. 31 (2): 140–153. doi:10.1016/j.biotechadv.2012.09.001. PMID 22985698.
- Taguchi S, Ooi T, Mizuno K, Matsusaki H (November 2015). "Advances and needs for endotoxin-free production strains". Applied Microbiology and Biotechnology. 99 (22): 9349–9360. doi:10.1007/s00253-015-6947-9. PMID 26362682. S2CID 8308134.
- Gerngross TU (November 2004). "Advances in the production of human therapeutic proteins in yeasts and filamentous fungi". Nature Biotechnology. 22 (11): 1409–1414. doi:10.1038/nbt1028. PMID 15529166. S2CID 22230030.
- Zhu J (2012). "Mammalian cell protein expression for biopharmaceutical production". Biotechnology Advances. 30 (5): 1158–1170. doi:10.1016/j.biotechadv.2011.08.022. PMID 21968146.
- Baeshen NA, Baeshen MN, Sheikh A, Bora RS, Ahmed MM, Ramadan HA, et al. (October 2014). "Cell factories for insulin production". Microbial Cell Factories. 13 (1): 141. doi:10.1186/s12934-014-0141-0. PMC 4203937. PMID 25270715.
- Jarvis DL (2009). "Chapter 14 Baculovirus–Insect Cell Expression Systems". Guide to Protein Purification, 2nd Edition. Methods in Enzymology. Vol. 463. Elsevier. pp. 191–222. doi:10.1016/s0076-6879(09)63014-7. ISBN 9780123745361. PMID 19892174.
- Galleno M, Sick AJ (1999). "Baculovirus expression vector system". Gene Expression Systems. Elsevier. pp. 331–363.
- "CERVARIX [Human Papillomavirus Bivalent (Types 16 and 18) Vaccine, Recombinant]". Food and Drug Administration.
- Wingfield PT (April 2015). "Overview of the purification of recombinant proteins". Current Protocols in Protein Science. 80 (1): 6.1.1–6.1.35. doi:10.1002/0471140864.ps0601s80. PMC 4410719. PMID 25829302.
- Shah RR (2017). "Overview of Vaccine Adjuvants: Introduction, History, and Current Status". In Fox CB, Hassett KJ, Brito LA (eds.). Vaccine Adjuvants. Methods in Molecular Biology. Vol. 1494. New York, NY: Springer New York. pp. 1–13. doi:10.1007/978-1-4939-6445-1_1. ISBN 978-1-4939-6443-7. PMID 27718182.
- Coffman RL, Sher A, Seder RA (October 2010). "Vaccine adjuvants: putting innate immunity to work". Immunity. 33 (4): 492–503. doi:10.1016/j.immuni.2010.10.002. PMC 3420356. PMID 21029960.
- Soler E, Houdebine LM (2007). "Preparation of recombinant vaccines". Biotechnology Annual Review. Elsevier. 13: 65–94. doi:10.1016/s1387-2656(07)13004-0. ISBN 978-0-444-53032-5. PMC 7106376. PMID 17875474.
- Rambe DS, Del Giudice G, Rossi S, Sanicas M (2015-07-06). "Safety and Mechanism of Action of Licensed Vaccine Adjuvants". International Current Pharmaceutical Journal. 4 (8): 420–431. doi:10.3329/icpj.v4i8.24024. ISSN 2224-9486.
- Qi F, Wu J, Li H, Ma G (2018-06-09). "Recent research and development of PLGA/PLA microspheres/nanoparticles: A review in scientific and industrial aspects". Frontiers of Chemical Science and Engineering. 13 (1): 14–27. doi:10.1007/s11705-018-1729-4. ISSN 2095-0179. S2CID 103993541.
- Vartak A, Sucheck SJ (April 2016). "Recent Advances in Subunit Vaccine Carriers". Vaccines. 4 (2): 12. doi:10.3390/vaccines4020012. PMC 4931629. PMID 27104575.
- Baxter D (December 2007). "Active and passive immunity, vaccine types, excipients and licensing". Occupational Medicine. 57 (8): 552–556. doi:10.1093/occmed/kqm110. PMID 18045976.
- Moyle PM, Toth I (March 2013). "Modern subunit vaccines: development, components, and research opportunities". ChemMedChem. 8 (3): 360–376. doi:10.1002/cmdc.201200487. PMID 23316023. S2CID 205647062.
- Vartak A, Sucheck SJ (April 2016). "Recent Advances in Subunit Vaccine Carriers". Vaccines. 4 (2): 12. doi:10.3390/vaccines4020012. PMC 4931629. PMID 27104575.
- Costa AP, Cobucci RN, da Silva JM, da Costa Lima PH, Giraldo PC, Gonçalves AK (2017). "Safety of Human Papillomavirus 9-Valent Vaccine: A Meta-Analysis of Randomized Trials". Journal of Immunology Research. 2017: 3736201. doi:10.1155/2017/3736201. PMC 5546048. PMID 28812030.
- Cox MM, Izikson R, Post P, Dunkle L (July 2015). "Safety, efficacy, and immunogenicity of Flublok in the prevention of seasonal influenza in adults". Therapeutic Advances in Vaccines. 3 (4): 97–108. doi:10.1177/2051013615595595. PMC 4591523. PMID 26478817.
- James SF, Chahine EB, Sucher AJ, Hanna C (July 2018). "Shingrix: The New Adjuvanted Recombinant Herpes Zoster Vaccine". The Annals of Pharmacotherapy. 52 (7): 673–680. doi:10.1177/1060028018758431. PMID 29457489. S2CID 206644211.
- "Possible Side effects from Vaccines". U.S. Centers for Disease Control and Prevention (CDC). 2022-04-06. Retrieved 2022-04-13.
- McNeil MM, DeStefano F (February 2018). "Vaccine-associated hypersensitivity". The Journal of Allergy and Clinical Immunology. 141 (2): 463–472. doi:10.1016/j.jaci.2017.12.971. PMC 6602527. PMID 29413255.
- Fink AL, Klein SL (November 2015). "Sex and Gender Impact Immune Responses to Vaccines Among the Elderly". Physiology. 30 (6): 408–416. doi:10.1152/physiol.00035.2015. PMC 4630198. PMID 26525340.
- Crowe JE (July 2007). "Genetic predisposition for adverse events after vaccination". The Journal of Infectious Diseases. 196 (2): 176–177. doi:10.1086/518800. PMID 17570102. S2CID 14121320.
- "ACIP Contraindications Guidelines for Immunization". U.S. Centers for Disease Control and Prevention (CDC). 2022-03-22. Retrieved 2022-04-14.
- Public Health Agency of Canada (2007-07-18). "Contraindications and precautions: Canadian Immunization Guide". www.canada.ca. Retrieved 2022-04-14.
- "RECOMBIVAX HB Hepatitis B Vaccine (Recombinant)" (PDF). Food and Drug Administration.
- "ENGERIX-B [Hepatitis B Vaccine (Recombinant)]" (PDF). Food and Drug Administration.
- Van Den Ende C, Marano C, Van Ahee A, Bunge EM, De Moerlooze L (August 2017). "The immunogenicity and safety of GSK's recombinant hepatitis B vaccine in adults: a systematic review of 30 years of experience". Expert Review of Vaccines. 16 (8): 811–832. doi:10.1080/14760584.2017.1338568. PMID 28573913. S2CID 4721288.
- "Gardasil[Human Papillomavirus Quadrivalent (Types 6, 11, 16, and 18) Vaccine, Recombinant]" (PDF). Food and Drug Administration.
- Gonçalves AK, Cobucci RN, Rodrigues HM, de Melo AG, Giraldo PC (2014). "Safety, tolerability and side effects of human papillomavirus vaccines: a systematic quantitative review". The Brazilian Journal of Infectious Diseases. 18 (6): 651–659. doi:10.1016/j.bjid.2014.02.005. PMC 9425215. PMID 24780368.
- "Gardasil-4 is no longer available". U.S. Centers for Disease Control and Prevention (CDC). 23 May 2022.
- Sagonowsky E (2016-10-21). "GSK exits U.S. market with its HPV vaccine Cervarix". Fierce Pharma. Retrieved 2022-03-15.
- O Murchu E, Comber L, Jordan K, Hawkshaw S, Marshall L, O'Neill M, et al. (February 2022). "Systematic review of the efficacy, effectiveness and safety of recombinant haemagglutinin seasonal influenza vaccines for the prevention of laboratory-confirmed influenza in individuals ≥18 years of age". Reviews in Medical Virology. 33 (3): e2331. doi:10.1002/rmv.2331. PMID 35106885. S2CID 246475234.
- Racine É, Gilca V, Amini R, Tunis M, Ismail S, Sauvageau C (September 2020). "A systematic literature review of the recombinant subunit herpes zoster vaccine use in immunocompromised 18-49 year old patients". Vaccine. 38 (40): 6205–6214. doi:10.1016/j.vaccine.2020.07.049. PMID 32788132. S2CID 221123883.
- Tricco AC, Zarin W, Cardoso R, Veroniki AA, Khan PA, Nincic V, et al. (October 2018). "Efficacy, effectiveness, and safety of herpes zoster vaccines in adults aged 50 and older: systematic review and network meta-analysis". BMJ. 363: k4029. doi:10.1136/bmj.k4029. PMC 6201212. PMID 30361202.
- "Nuvaxovid COVID-19 Vaccine (recombinant, adjuvanted)". 17 December 2021.
- Plotkin S (August 2014). "History of vaccination". Proceedings of the National Academy of Sciences of the United States of America. 111 (34): 12283–12287. Bibcode:2014PNAS..11112283P. doi:10.1073/pnas.1400472111. PMC 4151719. PMID 25136134.
- Noon JB, Aroian RV (December 2017). "Recombinant subunit vaccines for soil-transmitted helminths". Parasitology. 144 (14): 1845–1870. doi:10.1017/S003118201700138X. PMC 5729844. PMID 28770689.
- Marciani DJ, Kensil CR, Beltz GA, Hung CH, Cronier J, Aubert A (February 1991). "Genetically-engineered subunit vaccine against feline leukaemia virus: protective immune response in cats". Vaccine. 9 (2): 89–96. doi:10.1016/0264-410x(91)90262-5. PMID 1647576.
- Chen WH, Hotez PJ, Bottazzi ME (June 2020). "Potential for developing a SARS-CoV receptor-binding domain (RBD) recombinant protein as a heterologous human vaccine against coronavirus infectious disease (COVID)-19". Human Vaccines & Immunotherapeutics. 16 (6): 1239–1242. doi:10.1080/21645515.2020.1740560. PMC 7482854. PMID 32298218.