Ethylene glycol poisoning
Ethylene glycol poisoning is poisoning caused by drinking ethylene glycol.[1] Early symptoms include intoxication, vomiting and abdominal pain.[1] Later symptoms may include a decreased level of consciousness, headache, and seizures.[1] Long term outcomes may include kidney failure and brain damage.[1] Toxicity and death may occur after drinking even in a small amount[1] as ethylene glycol is more toxic than other diols.
| Ethylene glycol poisoning | |
|---|---|
| Other names | Ethylene glycol toxicity, ethylene glycol overdose |
 | |
| Ethylene glycol | |
| Specialty | Emergency medicine |
| Symptoms | Early: intoxication, vomiting, abdominal pain[1] Later: decreased level of consciousness, headache, seizures[1] |
| Complications | Kidney failure, brain damage[1] |
| Causes | Drinking ethylene glycol[1] |
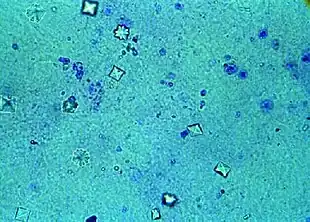
| Diagnostic method | Calcium oxalate crystals in the urine, acidosis or increased osmol gap in the blood[1] |
| Treatment | Antidote, hemodialysis[2] |
| Medication | Fomepizole, ethanol[2] |
| Frequency | > 5,000 cases per year (US)[3] |
Ethylene glycol is a colorless, odorless, sweet liquid, commonly found in antifreeze.[1] It may be drunk accidentally or intentionally in a suicide attempt.[2] When broken down by the body it results in glycolic acid and oxalic acid which cause most of the toxicity.[1][4] The diagnosis may be suspected when calcium oxalate crystals are seen in the urine or when acidosis or an increased osmol gap is present in the blood.[1] Diagnosis may be confirmed by measuring ethylene glycol levels in the blood; however, many hospitals do not have the ability to perform this test.[1]
Early treatment increases the chance of a good outcome.[2] Treatment consists of stabilizing the person, followed by the use of an antidote.[2] The preferred antidote is fomepizole with ethanol used if this is not available.[2] Hemodialysis may also be used in those where there is organ damage or a high degree of acidosis.[2] Other treatments may include sodium bicarbonate, thiamine, and magnesium.[2]
More than 5,000 cases of poisoning occur in the United States each year.[3] Those affected are often adults and male.[4] Deaths from ethylene glycol have been reported as early as 1930.[5] An outbreak of deaths in 1937 due to a medication mixed in a similar compound, diethylene glycol, resulted in the Food, Drug, and Cosmetic Act of 1938 in the United States, which mandated evidence of safety before new medications could be sold.[5] Antifreeze products sometimes have a substance to make them bitter added to discourage drinking by children or animals but this has not been found to be effective.[2]
Signs and symptoms
Signs of ethylene glycol poisoning depend upon the time after ingestion.[6] Symptoms usually follow a three-step progression, although poisoned individuals will not always develop each stage.[7][8]
- Stage 1 (30 minutes to 12 hours) consists of neurological and gastrointestinal symptoms and looks similar to alcohol poisoning.[9] Poisoned individuals may appear to be intoxicated, dizzy, lacking coordination of muscle movements, drooling, depressed,[6] and have slurred speech, seizures, abnormal eye movements, headaches, and confusion.[9] Irritation to the stomach may cause nausea and vomiting.[7] Also seen are excessive thirst and urination.[9] Over time, the body metabolizes ethylene glycol into other toxins.
- Stage 2 (12 to 36 hours) where signs of "alcohol" poisoning appear to resolve, underlying severe internal damage is still occurring.[9] An elevated heart rate, hyperventilation or increased breathing effort, and dehydration may start to develop, along with high blood pressure and metabolic acidosis.[9] These symptoms are a result of accumulation of organic acids formed by the metabolism of ethylene glycol. Additionally low calcium concentrations in the blood, overactive muscle reflexes, muscle spasms, QT interval prolongation, and congestive heart failure may occur. If untreated, death most commonly occurs during this period.[7]
- Stage 3 (24 to 72 hours) kidney failure is the result of ethylene glycol poisoning. In cats, this stage occurs 12–24 hours after consuming antifreeze; in dogs, at 36–72 hours after consuming antifreeze.[9] During this stage, severe kidney failure is developing secondary to calcium oxalate crystals forming in the kidneys.[9] Severe lethargy, coma, depression, vomiting, seizures, drooling, and inappetence may be seen.[9] Other symptoms include acute tubular necrosis, red blood cells in the urine, excess proteins in the urine, lower back pain, decreased or absent production of urine, elevated blood concentration of potassium, and acute kidney failure.[10][11] If kidney failure occurs it is typically reversible, although weeks or months of supportive care including hemodialysis may be required before kidney function returns.[7]
Sources
The most common source of ethylene glycol is automotive antifreeze or radiator coolant, where concentrations are high.[9] Other sources of ethylene glycol include windshield deicing agents, brake fluid, motor oil, developing solutions for hobby photographers, wood stains, solvents, and paints.[9] Some people put antifreeze into their cabin's toilet to prevent it from freezing during the winter, resulting in toxicities when animals drink from the toilet.[9] Small amounts of ethylene glycol may be contained in holiday ornaments such as snow globes.[9]
The most significant source of ethylene glycol is from aircraft de-icing and anti-icing operations, where it is released onto land and eventually to waterways near airports experiencing cold winter climates.[12] It is also used in manufacturing polyester products.[12] In 2006, approximately 1540 kilotonnes of ethylene glycol were manufactured in Canada by three companies in Alberta, with most of the production destined for export.[12]
Pathophysiology
The three main systems affected by ethylene glycol poisoning are the central nervous system, metabolic processes, and the kidneys.[7] The central nervous system is affected early in the course of poisoning as the result of a direct action of ethylene glycol. Similar to ethanol, it causes intoxication, followed by drowsiness or coma.[7] Seizures may occur due to a direct effect.[10] The toxic mechanism of ethylene glycol poisoning is mainly due to the metabolites of ethylene glycol. Initially it is metabolized by alcohol dehydrogenase to glycolaldehyde, which is then oxidized to glycolic acid by aldehyde dehydrogenase.[7]
The increase in metabolites may cause encephalopathy or cerebral edema.[13] The metabolic effects occur 12 to 36 hours post ingestion, causing primarily metabolic acidosis which is due mainly to accumulated glycolic acid. Additionally, as a side effect of the first two steps of metabolism, an increase in the blood concentration of lactic acid occurs contributing to lactic acidosis. The formation of acid metabolites also causes inhibition of other metabolic pathways, such as oxidative phosphorylation.[7]
The kidney toxicity of ethylene glycol occurs 24 to 72 hours post ingestion and is caused by a direct cytotoxic effect of glycolic acid. The glycolic acid is then metabolized to glyoxylic acid and finally to oxalic acid. Oxalic acid binds with calcium to form calcium oxalate crystals which may deposit and cause damage to many areas of the body including the brain, heart, kidneys, and lungs.[7] The most significant effect is accumulation of calcium oxalate crystals in the kidneys which causes kidney damage leading to oliguric or anuric acute kidney failure.[7] The rate-limiting step in this cascade is the conversion of glycolic to glyoxylic acid.[14] Accumulation of glycolic acid in the body is mainly responsible for toxicity.[15]
Toxicity
Ethylene glycol has been shown to be toxic to humans[16] and is also toxic to domestic pets such as cats and dogs. A toxic dose requiring medical treatment varies but is considered more than 0.1 mL per kg body weight (mL/kg) of pure substance. That is roughly 16 mL of 50% ethylene glycol for an 80 kg adult and 4 mL for a 20 kg child. Poison control centers often use more than a lick or taste in a child or more than a mouthful in an adult as a dose requiring hospital assessment.[17]
The orally lethal dose in humans has been reported as approximately 1.4 mL/kg of pure ethylene glycol.[7] That is approximately 224 mL (7.6 oz.) of 50% ethylene glycol for an 80 kg adult and 56 mL (2 oz.) for a 20 kg child. Although survival with medical treatment has occurred with doses much higher than this, death has occurred with 30 mL of the concentrate in an adult.[18][19][20] In the EU classification of dangerous substances it is 'harmful' (Xn) while more toxic substances are classified as 'toxic' (T) or 'very toxic' (T+). The U.S. Environmental Protection Agency generally puts substances which are lethal at more than 30 g to adults in Toxicity Class III.
Ethylene glycol has a low vapor pressure; it does not evaporate readily at normal temperatures and therefore high concentrations in air or intoxication are unlikely to occur following inhalational exposures.[21] There may be a slight risk of poisoning where mists or fogs are generated, although this rarely leads to poisoning as ethylene glycol causes irritation and coughing when breathed in, alerting victims to its presence.[22] Ethylene glycol is not well absorbed through skin meaning poisoning following dermal exposure is also uncommon.[23]
Diagnosis
As many of the clinical signs and symptoms of ethylene glycol poisoning are nonspecific and occur in many poisonings; the diagnosis is often difficult.[24] It is most reliably diagnosed by the measurement of the blood ethylene glycol concentration. Ethylene glycol in biological fluids can be determined by gas chromatography.[25] Many hospital laboratories do not have the ability to perform this blood test and in the absence of this test the diagnosis must be made based on the presentation of the person.[7]
In this situation a helpful test to diagnose poisoning is the measurement of the osmolal gap. The person' serum osmolality is measured by freezing point depression and then compared with the predicted osmolality based on the person's measured sodium, glucose, blood urea nitrogen, and any ethanol that may have been ingested. The presence of a large osmolal gap supports a diagnosis of ethylene glycol poisoning. However, a normal osmolar gap does not rule out ethylene glycol exposure because of wide individual variability.[26][27]
The increased osmolal gap is caused by the ethylene glycol itself. As the metabolism of ethylene glycol progresses there will be less ethylene glycol and this will decrease the blood ethylene glycol concentration and the osmolal gap making this test less useful.[28] Additionally, the presence of other alcohols such as ethanol, isopropanol, or methanol or conditions such as alcoholism or diabetic ketoacidosis, lactic acidosis, or kidney failure may also produce an elevated osmolal gap leading to a false diagnosis.[7]
Other laboratory abnormalities may suggest poisoning, especially the presence of a metabolic acidosis, particularly if it is characterized by a large anion gap. Large anion gap acidosis is usually present during the initial stage of poisoning. However, acidosis has a large number of differential diagnoses, including poisoning from methanol, salicylates, iron, isoniazid, paracetamol, theophylline, or from conditions such as uremia or diabetic and alcoholic ketoacidosis.
The diagnosis of ethylene glycol poisoning should be considered in any people with a severe acidosis.[7] Urine microscopy can reveal needle or envelope-shaped calcium oxalate crystals in the urine which can suggest poisoning; although these crystals may not be present until the late stages of poisoning.[29] Finally, many commercial radiator antifreeze products have fluorescein added to enable radiator leaks to be detected using a Wood's lamp. Following ingestion of antifreeze products containing ethylene glycol and fluorescein, a Wood's lamp may reveal fluorescence of a person's mouth area, clothing, vomitus, or urine which can help to diagnose poisoning.[30][31]
Prevention
Antifreeze products for automotive use containing propylene glycol in place of ethylene glycol are available, and are generally considered safer to use, as it possesses an unpleasant taste in contrast to the perceived "sweet" taste of toxic ethylene glycol-based coolants, and produces only lactic acid in an animal's body, as their muscles do when exercised.[32]
When using antifreeze products containing ethylene glycol, recommended safety measures include:
- Cleaning up any spill immediately[33] and thoroughly. Spills may be cleaned by sprinkling cat litter, sand or other absorbent material directly on the spill.[34] Once fully absorbed, while wearing protective gloves, the material may be scooped into a plastic bag, sealed and disposed.[34] The spill area may be scrubbed with a stiff brush and warm, soapy water.[34] The soapy water is not recommended to be drained in a storm drain.[34]
- Checking vehicles regularly for leaks.[33]
- Storing antifreeze in clearly marked original sealed containers, in areas that are inaccessible to pets[33] or small children.[34]
- Keeping pets and small children away from the area when draining the car radiator.[33]
- Disposing of used antifreeze only by taking to a service station.[34]
- If antifreeze is placed in toilets, ensuring the lid is down and the door closed.[6]
Treatment
Stabilization and decontamination
The most important initial treatment for ethylene glycol poisoning is stabilizing the person. As ethylene glycol is rapidly absorbed, gastric decontamination is unlikely to be of benefit unless it is performed within 60 minutes of ingestion. Traditionally, gastric lavage or nasogastric aspiration of gastric contents are the most common methods employed in ethylene glycol poisoning.[7] The usefulness of gastric lavage has, however, been questioned, and it is now no longer used routinely in poisoning situations.[35] Ipecac-induced vomiting is not recommended. As activated charcoal does not adsorb glycols, it is not recommended as it will not be effective at preventing absorption.[7] It is only used in the presence of a toxic dose of another poison or drug.[26] People with significant poisoning often present in a critical condition. In this situation stabilization of the person including airway management with intubation should be performed in preference to gastrointestinal decontamination.[7] People presenting with metabolic acidosis or seizures require treatment with sodium bicarbonate and anticonvulsives such as a benzodiazepine respectively.[7] Sodium bicarbonate should be used cautiously as it can worsen hypocalcemia by increasing the plasma protein binding of calcium. If hypocalcemia occurs it can be treated with calcium replacement although calcium supplementation can increase the precipitation of calcium oxalate crystals leading to tissue damage.[24] Intubation and respiratory support may be required in severely intoxicated people; people with hypotension require treatment with intravenous fluids and possibly vasopressors.[36]
Antidotes
Following decontamination and the institution of supportive measures, the next priority is inhibition of further ethylene glycol metabolism using antidotes. The antidotes for ethylene glycol poisoning are ethanol and fomepizole. This antidotal treatment forms the mainstay of management of ethylene glycol poisoning. The toxicity of ethylene glycol comes from its metabolism to glycolic acid and oxalic acid. The goal of pharmacotherapy is to prevent the formation of these metabolites. Ethanol acts by competing with ethylene glycol for alcohol dehydrogenase (ADH), the first enzyme in the degradation pathway. Because ethanol has nearly 100 times more affinity for ADH, it blocks the breakdown of ethylene glycol into glycolaldehyde, thus preventing further degradation to oxalic acid and the associated nephrotoxic effects. The unreacted ethylene glycol remains in the body and is eventually excreted in the urine; however, supportive therapy for the CNS depression and metabolic acidosis will be required until the ethylene glycol concentrations fall below toxic limits. Pharmaceutical grade ethanol is usually given intravenously as a 5 or 10% solution in 5% dextrose, but it is also sometimes given orally in the form of a strong spirit such as whisky, vodka, or gin.[7]
Fomepizole is a potent inhibitor of alcohol dehydrogenase; similar to ethanol, it acts to block the formation of the toxic metabolites.[24][36][37] Fomepizole has been shown to be highly effective as an antidote for ethylene glycol poisoning.[37][38] It is the only antidote approved by the U.S. Food and Drug Administration for the treatment of ethylene glycol poisoning.[7] Both antidotes have advantages and disadvantages. Ethanol is readily available in most hospitals, is inexpensive, and can be administered orally as well as intravenously. Its adverse effects include intoxication, hypoglycemia in children, and possible liver toxicity.[26] People receiving ethanol therapy also require frequent blood ethanol concentration measurements and dosage adjustments to maintain a therapeutic ethanol concentration. People therefore must be monitored in an intensive care unit. Alternatively, the adverse side effects of fomepizole are minimal and the approved dosing regimen maintains therapeutic concentrations without the need to monitor blood concentrations of the drug. The disadvantage of fomepizole is that it is expensive. Costing US$1,000 per gram, an average course used in an adult poisoning would cost approximately $3,500 to $4,000.[39][40] Despite the cost, fomepizole is gradually replacing ethanol as the antidote of choice in ethylene glycol poisoning.[37][38]
Adjunct agents including thiamine and pyridoxine are often given, because they may help prevent the formation of oxalic acid.[7] The use of these agents is based on theoretical observations and there is limited evidence to support their use in treatment; they may be of particular benefit in people who could be deficient in these vitamins such as those who are malnourished or alcoholic.[24]
Hemodialysis
In addition to antidotes, an important treatment for poisoning is the use of hemodialysis. Hemodialysis is used to enhance the removal of unmetabolized ethylene glycol, as well as its metabolites from the body. It has been shown to be highly effective in the removal of ethylene glycol and its metabolites from the blood.[14][41] Hemodialysis also has the added benefit of correcting other metabolic derangements or supporting deteriorating kidney function. Hemodialysis is usually indicated in people with severe metabolic acidosis (blood pH less than 7.3), kidney failure, severe electrolyte imbalance, or if the person's condition is deteriorating despite treatment.[10][24] Often both antidotal treatment and hemodialysis are used together in the treatment of poisoning. Because hemodialysis will also remove the antidotes from the blood, doses of antidotes need to be increased to compensate.[7] If hemodialysis is not available, then peritoneal dialysis also removes ethylene glycol, although less efficiently.[42]
Prognosis
Treatment for antifreeze poisoning needs to be started as soon after ingestion as possible to be effective; the earlier treatment is started, the greater the chance of survival.[6][43] Cats must be treated within 3 hours of ingesting of antifreeze to be effective, while dogs must be treated within 8–12 hours of ingestion.[9] Once kidney failure develops, the prognosis is poor.[9]
Generally, if the person is treated and survives then a full recovery is expected.[44] People who present early to medical facilities and have prompt medical treatment typically will have a favorable outcome.[45] Alternatively, people presenting late with signs and symptoms of coma, hyperkalemia, seizures, or severe acidosis have a poor prognosis.[17] People who develop severe central nervous system manifestations or stroke who survive may have long term neurologic dysfunction; in some cases they may recover, although convalescence may be prolonged.[46][47][48][49] The most significant long-term complication is related to the kidneys. Cases of permanent kidney damage, often requiring chronic dialysis or kidney transplantation, have been reported after severe poisoning.[50][51]
Epidemiology
Ethylene glycol poisoning is a relatively common occurrence worldwide.[51][52][53][54] Human poisoning often occurs in isolated cases, but may also occur in epidemics.[55][56][57] Many cases of poisoning are the result of using ethylene glycol as a cheap substitute for alcohol or intentional ingestions in suicide attempts.[44] Less commonly it has been used as a means of homicide.[58][59] Children or animals may be exposed by accidental ingestion; children and animals often consume large amounts due to ethylene glycol having a sweet taste.[60] In the United States there were 5816 cases reported to poison centers in 2002.[17] Additionally, ethylene glycol was the most common chemical responsible for deaths reported by US poison centers in 2003.[52] In Australia there were 17 cases reported to the Victorian poison center and 30 cases reported to the New South Wales poison center in 2007.[61][62] However, these numbers may underestimate actual numbers because not all cases attributable to ethylene glycol are reported to poison control centers.[63] Most deaths from ethylene glycol are intentional suicides; deaths in children due to unintentional ingestion are extremely rare.[64]
In an effort to prevent poisoning, often a bittering agent called denatonium benzoate, known by the trade name Bitrex, is added to ethylene glycol preparations as an adversant to prevent accidental or intentional ingestion. The bittering agent is thought to stop ingestion as part of the human defense against ingestion of harmful substances is rejection of bitter tasting substances.[65] In the United States, eight states (Oregon, California, New Mexico, Virginia, Arizona, Maine, Tennessee, Washington) have made the addition of bittering agents to antifreeze compulsory.[64][66][67] Three follow up studies targeting limited populations or suicidal persons to assess the efficacy of bittering agents in preventing toxicity or death have, however, shown limited benefit of bittering ethylene glycol preparations in these two populations.[64][68][69] Specifically, Mullins finds that bittering of antifreeze does not reduce reported cases of poisoning of preschoolers in the US state of Oregon.[68] Similarly, White found that adding bittering agents did not decrease the frequency or severity of antifreeze poisonings in children under the age of 5.[69] Additionally, another study by White found that suicidal persons are not deterred by the bittered taste of antifreeze in their attempts to kill themselves.[64] These studies did not focus on poisoning of domestic pets or livestock, for example, or inadvertent exposure to bittered antifreeze among a large population (of non-preschool age children).
Poisoning of a raccoon was diagnosed in 2002 in Prince Edward Island, Canada.[70] An online veterinary manual provides information on lethal doses of ethylene glycol for chicken, cattle, as well as cats and dogs, adding that younger animals may be more susceptible.[71]
History
Ethylene glycol was once thought innocuous; in 1931 it was suggested as being suitable for use as a vehicle or solvent for injectable pharmaceutical preparations.[72] Numerous cases of poisoning have been reported since then, and it has been shown to be toxic to humans.[16]
Environmental effects
Ethylene glycol involved in aircraft de-icing and anti-icing operations is released onto land and eventually to waterways.[12] A report prepared for the World Health Organization in 2000 stated that laboratory tests exposing aquatic organisms to stream water receiving runoff from airports have shown toxic effects and death (p. 12).[73] Field studies in the vicinity of an airport have reported toxic signs consistent with ethylene glycol poisoning, fish kills, and reduced biodiversity, although those effects could not definitively be ascribed to ethylene glycol (p. 12).[73] The process of biodegrading of glycols also increases the risk to organisms, as oxygen levels become depleted in surface waters (p. 13).[73] Another study found the toxicity to aquatic and other organisms was relatively low, but the oxygen-depletion effect of biodegradation was more serious (p. 245).[74] Further, "Anaerobic biodegradation may also release relatively toxic byproducts such as acetaldehyde, ethanol, acetate, and methane (p. 245)."[74]
In Canada, Environment Canada reports that "in recent years, management practices at Canada’s major airports have improved with the installation of new ethylene glycol application and mitigation facilities or improvements to existing ones."[12] Since 1994, federal airports must comply with the Glycol Guidelines of the Canadian Environmental Protection Act, monitoring and reporting on concentrations of glycols in surface water.[75] Detailed mitigation plans include storage and handling issues (p. 27), spill response procedures, and measures taken to reduce volumes of fluid (p. 28).[76] Considering factors such as the "seasonal nature of releases, ambient temperatures, metabolic rates and duration of exposure", Environment Canada stated in 2014 that "it is proposed that ethylene glycol is not entering the environment in a quantity or concentration or under conditions that have or may have an immediate or long-term harmful effect on the environment or its biological diversity".[12]
In the U.S., airports are required to obtain stormwater discharge permits and ensure that wastes from deicing operations are properly collected and treated.[77] Large new airports may be required to collect 60 percent of aircraft deicing fluid after deicing.[77] Airports that discharge the collected aircraft deicing fluid directly to waters of the U.S. must also meet numeric discharge requirements for chemical oxygen demand.[77] A report in 2000 stated that ethylene glycol was becoming less popular for aircraft deicing in the U.S., due to its reporting requirements and adverse environmental impacts (p. 213), and noted a shift to the use of propylene glycol (p. I-3).[74]
Other animals
Once kidney failure has developed in dogs and cats, the outcome is poor.[9] The treatment is generally the same, although vodka or rectified spirits may be substituted for pharmaceutical grade ethanol in IV injections.[78]
See also
- Methylmalonic acidemia – an autosomal recessive metabolic disorder that mimics the effects of ethylene glycol poisoning.
- 1985 diethylene glycol wine scandal
- Elixir sulfanilamide, a banned medicine that caused mass poisoning because it used ethylene glycol as a solvent
- Methanol poisoning
References
- Kruse, JA (October 2012). "Methanol and ethylene glycol intoxication". Critical Care Clinics. 28 (4): 661–711. doi:10.1016/j.ccc.2012.07.002. PMID 22998995.
- Beauchamp, GA; Valento, M (September 2016). "Toxic Alcohol Ingestion: Prompt Recognition And Management In The Emergency Department". Emergency Medicine Practice. 18 (9): 1–20. PMID 27538060.
- Naidich, Thomas P.; Castillo, Mauricio; Cha, Soonmee; Smirniotopoulos, James G. (2012). Imaging of the Brain: Expert Radiology Series. Elsevier Health Sciences. p. 960. ISBN 978-0323186476. Archived from the original on 2017-09-08.
- Ferri, Fred F. (2016). Ferri's Clinical Advisor 2017: 5 Books in 1. Elsevier Health Sciences. p. 794. ISBN 9780323448383. Archived from the original on 2017-09-08.
- Shaw, Leslie M. (2001). The Clinical Toxicology Laboratory: Contemporary Practice of Poisoning Evaluation. Amer. Assoc. for Clinical Chemistry. p. 197. ISBN 9781890883539. Archived from the original on 2017-09-08.
- "College of Veterinary Medicine: Pet Health Topics: Antifreeze Poisoning" Archived 2015-02-10 at the Wayback Machine, Washington State University, accessed Sept. 11, 2014.
- Brent J (2001). "Current management of ethylene glycol poisoning". Drugs. 61 (7): 979–88. doi:10.2165/00003495-200161070-00006. ISSN 0012-6667. PMID 11434452. S2CID 22954381.
- Hess, R; Bartels, MJ; Pottenger, LH (December 2004). "Ethylene glycol: an estimate of tolerable levels of exposure based on a review of animal and human data" (PDF). Archives of Toxicology. 78 (12): 671–80. doi:10.1007/s00204-004-0594-8. PMID 15372138. S2CID 19995896.
- "Antifreeze Poisoning in Dogs & Cats (Ethylene Glycol Poisoning)" Archived 2014-09-12 at the Wayback Machine, Pet Poison Helpline, accessed Sept. 11, 2014.
- Barceloux DG, Krenzelok EP, Olson K, Watson W (1999). "American Academy of Clinical Toxicology Practice Guidelines on the Treatment of Ethylene Glycol Poisoning. Ad Hoc Committee". Journal of Toxicology: Clinical Toxicology. 37 (5): 537–60. doi:10.1081/CLT-100102445. ISSN 0731-3810. PMID 10497633.
- Bobbitt WH, Williams RM, Freed CR (February 1986). "Severe ethylene glycol intoxication with multisystem failure". Western Journal of Medicine. 144 (2): 225–8. ISSN 0093-0415. PMC 1306577. PMID 3953092.
- "Government of Canada: Environment Canada: Ethylene Glycol (Final Content)" Archived 2014-09-13 at the Wayback Machine, April 16, 2014.
- Maier W (1983). "Cerebral computed tomography of ethylene glycol intoxication". Neuroradiology. 24 (3): 175–7. doi:10.1007/BF00347839. ISSN 0028-3940. PMID 6828232. S2CID 9038812.
- Gabow PA, Clay K, Sullivan JB, Lepoff R (July 1986). "Organic acids in ethylene glycol intoxication". Annals of Internal Medicine. 105 (1): 16–20. doi:10.7326/0003-4819-105-1-16. ISSN 0003-4819. PMID 3717806.
- Clay KL, Murphy RC (January 1977). "On the metabolic acidosis of ethylene glycol intoxication". Toxicology and Applied Pharmacology. 39 (1): 39–49. doi:10.1016/0041-008X(77)90175-2. ISSN 0041-008X. PMID 14421.
- Friedman EA, Greenberg JB, Merrill JP, Dammin GJ (June 1962). "Consequences of ethylene glycol poisoning. Report of four cases and review of the literature". The American Journal of Medicine. 32 (6): 891–902. doi:10.1016/0002-9343(62)90035-9. ISSN 0002-9343. PMID 13895244.
- Caravati EM, Erdman AR, Christianson G, et al. (2005). "Ethylene glycol exposure: an evidence-based consensus guideline for out-of-hospital management". Clinical Toxicology. 43 (5): 327–45. doi:10.1080/07313820500184971. ISSN 1556-3650. PMID 16235508. S2CID 2672302.
- Eder AF, McGrath CM, Dowdy YG, Tomaszewski JE, Rosenberg FM, Wilson RB, Wolf BA, Shaw LM (January 1998). "Ethylene glycol poisoning: toxicokinetic and analytical factors affecting laboratory diagnosis". Clinical Chemistry. 44 (1): 168–77. doi:10.1093/clinchem/44.1.168. ISSN 0009-9147. PMID 9550575.
- Field DL (October 1985). "Acute ethylene glycol poisoning". Critical Care Medicine. 13 (10): 872–3. doi:10.1097/00003246-198510000-00024. ISSN 0090-3493. PMID 4028762.
- Amathieu R, Merouani M, Borron SW, Lapostolle F, Smail N, Adnet F (August 2006). "Prehospital diagnosis of massive ethylene glycol poisoning and use of an early antidote". Resuscitation. 70 (2): 285–6. doi:10.1016/j.resuscitation.2005.12.014. ISSN 0300-9572. PMID 16808995.
- Hodgman MJ, Wezorek C, Krenzelok E (1997). "Toxic inhalation of ethylene glycol: a pharmacological improbability". Journal of Toxicology: Clinical Toxicology. 35 (1): 109–11. doi:10.3109/15563659709001176. PMID 9022663.
- Wills JH, Coulston F, Harris ES, McChesney EW, Russell JC, Serrone DM (1974). "Inhalation of aerosolized ethylene glycol by man". Clinical Toxicology. 7 (5): 463–76. doi:10.3109/15563657408988020. ISSN 0009-9309. PMID 4613525.
- Driver J, Tardiff RG, Sedik L, Wester RC, Maibach HI (July 1993). "In vitro percutaneous absorption of [14C] ethylene glycol". Journal of Exposure Analysis and Environmental Epidemiology. 3 (3): 277–84. ISSN 1053-4245. PMID 8260837.
- Hall TL (May 2002). "Fomepizole in the treatment of ethylene glycol poisoning" (PDF). Canadian Journal of Emergency Medical Care. 4 (3): 199–204. doi:10.1017/s1481803500006382. ISSN 1481-8035. PMID 17609006. S2CID 6058769. Archived from the original (PDF) on 2012-07-27.
- Aarstad K, Dale O, Aakervik O, Ovrebø S, Zahlsen K (July 1993). "A rapid gas chromatographic method for determination of ethylene glycol in serum and urine". Journal of Analytical Toxicology. 17 (4): 218–21. doi:10.1093/jat/17.4.218. ISSN 0146-4760. PMID 8371550.
- Jacobsen D, McMartin KE (1997). "Antidotes for methanol and ethylene glycol poisoning". Journal of Toxicology: Clinical Toxicology. 35 (2): 127–43. doi:10.3109/15563659709001182. ISSN 0731-3810. PMID 9120880.
- Hoffman RS, Smilkstein MJ, Howland MA, Goldfrank LR (1993). "Osmol gaps revisited: normal values and limitations". Journal of Toxicology: Clinical Toxicology. 31 (1): 81–93. doi:10.3109/15563659309000375. ISSN 0731-3810. PMID 8433417.
- Glaser DS (March 1996). "Utility of the serum osmol gap in the diagnosis of methanol or ethylene glycol ingestion". Annals of Emergency Medicine. 27 (3): 343–6. doi:10.1016/S0196-0644(96)70271-8. ISSN 0196-0644. PMID 8599495.
- Jacobsen D, Akesson I, Shefter E (May 1982). "Urinary calcium oxalate monohydrate crystals in ethylene glycol poisoning". Scandinavian Journal of Clinical and Laboratory Investigation. 42 (3): 231–4. doi:10.3109/00365518209168078. ISSN 0036-5513. PMID 7134806.
- Winter ML, Ellis MD, Snodgrass WR (June 1990). "Urine fluorescence using a Wood's lamp to detect the antifreeze additive sodium fluorescein: a qualitative adjunctive test in suspected ethylene glycol ingestions". Annals of Emergency Medicine. 19 (6): 663–7. doi:10.1016/S0196-0644(05)82472-2. ISSN 0196-0644. PMID 2344083.
- Wallace KL, Suchard JR, Curry SC, Reagan C (July 2001). "Diagnostic use of physicians' detection of urine fluorescence in a simulated ingestion of sodium fluorescein-containing antifreeze". Annals of Emergency Medicine. 38 (1): 49–54. doi:10.1067/mem.2001.115531. ISSN 0196-0644. PMID 11423812.
- Pieter Klapwijk (January 27, 2010). "Ethylene Glycol Poisoning". The Rested Dog Inn. Archived from the original on January 26, 2013. Retrieved October 11, 2012.
- "Oklahoma Veterinary Medical Association: ASPCA answers questions about antifreeze poisoning" Archived 2016-03-04 at the Wayback Machine, accessed Sept. 11, 2014.
- J.J. Mackenzie, "Prevent Antifreeze Poisoning", in Laurie Halse Anderson, Vet Volunteers: Acting Out (2012), Puffin Books, ISBN 9780142416761, p. 125.
- Vale JA, Kulig K (2004). "Position paper: gastric lavage". Journal of Toxicology: Clinical Toxicology. 42 (7): 933–43. doi:10.1081/CLT-200045006. ISSN 0731-3810. PMID 15641639. S2CID 29957973.
- Brent J (May 2009). "Fomepizole for ethylene glycol and methanol poisoning". The New England Journal of Medicine. 360 (21): 2216–23. doi:10.1056/NEJMct0806112. ISSN 0028-4793. PMID 19458366. S2CID 33354715.
- Brent J, McMartin K, Phillips S, Burkhart K, Donovan J, Wells M, Kulig K (March 1999). "Fomepizole for the treatment of ethylene glycol poisoning. Methylpyrazole for Toxic Alcohols Study Group". The New England Journal of Medicine. 340 (11): 832–8. doi:10.1056/NEJM199903183401102. ISSN 0028-4793. PMID 10080845.
- Borron SW, Mégarbane B, Baud FJ (September 1999). "Fomepizole in treatment of uncomplicated ethylene glycol poisoning". The Lancet. 354 (9181): 831. doi:10.1016/S0140-6736(99)80015-4. ISSN 0140-6736. PMID 10485727. S2CID 45856395.
- Shannon M (April 1998). "Toxicology reviews: fomepizole--a new antidote". Pediatric Emergency Care. 14 (2): 170–2. doi:10.1097/00006565-199804000-00021. ISSN 0749-5161. PMID 9583406.
- Scalley RD, Ferguson DR, Piccaro JC, Smart ML, Archie TE (September 2002). "Treatment of ethylene glycol poisoning" (Free full text). American Family Physician. 66 (5): 807–12. ISSN 0002-838X. PMID 12322772.
- Moreau CL, Kerns W, Tomaszewski CA, McMartin KE, Rose SR, Ford MD, Brent J (1998). "Glycolate kinetics and hemodialysis clearance in ethylene glycol poisoning. META Study Group". Journal of Toxicology: Clinical Toxicology. 36 (7): 659–66. doi:10.3109/15563659809162613. ISSN 0731-3810. PMID 9865233.
- Aakervik O, Svendsen J, Jacobsen D (October 2002). "[Severe ethylene glycol poisoning treated with fomepizole (4-methylpyrazole)]". Tidsskrift for den Norske Lægeforening (in Norwegian). 122 (25): 2444–6. ISSN 0029-2001. PMID 12448112.
- Eder Anne F.; et al. (1998). "Ethylene glycol poisoning: toxicokinetic and analytical factors affecting laboratory diagnosis". Clinical Chemistry. 44 (1): 168–177. doi:10.1093/clinchem/44.1.168. PMID 9550575. Archived from the original on 2014-12-03.
- Leth PM, Gregersen M (December 2005). "Ethylene glycol poisoning". Forensic Science International. 155 (2–3): 179–84. doi:10.1016/j.forsciint.2004.11.012. ISSN 0379-0738. PMID 16226155.
- Velez LI, Shepherd G, Lee YC, Keyes DC (September 2007). "Ethylene glycol ingestion treated only with fomepizole". Journal of Medical Toxicology. 3 (3): 125–8. doi:10.1007/BF03160922. ISSN 1556-9039. PMC 3550067. PMID 18072148.
- Jacobsen D, McMartin KE (September 1986). "Methanol and ethylene glycol poisonings. Mechanism of toxicity, clinical course, diagnosis and treatment". Medical Toxicology. 1 (5): 309–34. doi:10.1007/bf03259846. ISSN 0112-5966. PMID 3537623. S2CID 25188780.
- Berger JR, Ayyar DR (November 1981). "Neurological complications of ethylene glycol intoxication. Report of a case". Archives of Neurology. 38 (11): 724–6. doi:10.1001/archneur.1981.00510110084016. ISSN 0003-9942. PMID 7305705.
- Lewis LD, Smith BW, Mamourian AC (June 1997). "Delayed sequelae after acute overdoses or poisonings: cranial neuropathy related to ethylene glycol ingestion". Clinical Pharmacology & Therapeutics. 61 (6): 692–9. doi:10.1016/S0009-9236(97)90105-3. ISSN 0009-9236. PMID 9209253. S2CID 23994655.
- Spillane L, Roberts JR, Meyer AE (February 1991). "Multiple cranial nerve deficits after ethylene glycol poisoning". Annals of Emergency Medicine. 20 (2): 208–10. doi:10.1016/S0196-0644(05)81226-0. ISSN 0196-0644. PMID 1996809.
- Nizze H, Schwabbauer P, Brachwitz C, Lange H (July 1997). "[Fatal chronic oxalosis after sublethal ethylene glycol poisoning]". Der Pathologe (in German). 18 (4): 328–34. doi:10.1007/s002920050224. ISSN 0172-8113. PMID 9380607. S2CID 10496499. Archived from the original on 2000-10-02.
- Davis DP, Bramwell KJ, Hamilton RS, Williams SR (September 1997). "Ethylene glycol poisoning: case report of a record-high level and a review". The Journal of Emergency Medicine. 15 (5): 653–67. doi:10.1016/S0736-4679(97)00145-5. ISSN 0736-4679. PMID 9348055.
- Watson WA, Litovitz TL, Klein-Schwartz W, Rodgers GC Jr, Youniss J, Reid N, Rouse WG, Rembert RS, Borys D (September 2004). "2003 annual report of the American Association of Poison Control Centers Toxic Exposure Surveillance System". American Journal of Emergency Medicine. 22 (5): 335–404. doi:10.1016/j.ajem.2004.06.001. ISSN 0735-6757. PMID 15490384.
- Kotwica M, Czerczak S (2007). "Acute poisonings registered since 1970: trends and characteristics. Analysis of the files collected in the National Poison Information Centre, Łódź, Poland". International Journal of Occupational Medicine and Environmental Health. 20 (1): 38–43. doi:10.2478/v10001-007-0010-8. ISSN 1232-1087. PMID 17509968.
- Krenová M, Pelclová D, Navrátil T, Merta M (December 2005). "Experiences of the Czech toxicological information centre with ethylene glycol poisoning" (PDF). Biomedical Papers of the Medical Faculty of the University Palacký, Olomouc, Czechoslovakia. 149 (2): 473–5. doi:10.5507/bp.2005.083. ISSN 1213-8118. PMID 16601813. Archived from the original (PDF) on 2009-03-06.
- Centers for Disease Control (CDC) (September 1987). "Ethylene glycol intoxication due to contamination of water systems". MMWR. Morbidity and Mortality Weekly Report. 36 (36): 611–4. ISSN 0149-2195. PMID 3114608.
- Leikin JB, Toerne T, Burda A, McAllister K, Erickson T (November 1997). "Summertime cluster of intentional ethylene glycol ingestions". JAMA: The Journal of the American Medical Association. 278 (17): 1406. doi:10.1001/jama.278.17.1406. ISSN 0098-7484. PMID 9355997.
- Goldsher M, Better OS (May 1979). "Antifreeze poisoning during the October 1973 War in the Middle-East: case reports". Military Medicine. 144 (5): 314–5. doi:10.1093/milmed/144.5.314. ISSN 0026-4075. PMID 113700.
- Armstrong EJ, Engelhart DA, Jenkins AJ, Balraj EK (June 2006). "Homicidal ethylene glycol intoxication: a report of a case". The American Journal of Forensic Medicine and Pathology. 27 (2): 151–5. doi:10.1097/01.paf.0000203221.17854.38. ISSN 0195-7910. PMID 16738434. S2CID 26053725.
- Munro, Ian (October 13, 2007). "Death by anti-freeze 'perfect murder'". The Age. Archived from the original on January 18, 2008. Retrieved 2008-10-01.
- Goldfrank LR, Flomenbaum NE, Lewin NA, Howland MA, Hoffman RS, Nelson LS, eds. (2002). Goldfrank's toxicologic emergencies. McGraw-Hill. pp. 980–90. ISBN 978-0-07-136001-2. OCLC 48177200.
- "Annual Report 2007" (PDF). Victorian Poisons Information Centre. 2008. Archived from the original (PDF) on 2011-02-24. Retrieved 2008-10-12.
- "Annual Report 2007" (PDF). New South Wales Poisons Information Centre. 2008. Archived from the original (PDF) on August 2, 2008. Retrieved 2008-10-12.
- LaKind JS, McKenna EA, Hubner RP, Tardiff RG (July 1999). "A review of the comparative mammalian toxicity of ethylene glycol and propylene glycol". Critical Reviews in Toxicology. 29 (4): 331–65. doi:10.1080/10408449991349230. ISSN 1040-8444. PMID 10451263.
- White NC, Litovitz T, White MK, Watson WA, Benson BE, Horowitz BZ, Marr-Lyon L (July 2008). "The impact of bittering agents on suicidal ingestions of antifreeze". Clinical Toxicology. 46 (6): 507–14. doi:10.1080/15563650802119700. ISSN 1556-3650. PMID 18584362. S2CID 205901974.
- Jackson MH, Payne HA (August 1995). "Bittering agents: their potential application in reducing ingestions of engine coolants and windshield wash". Veterinary and Human Toxicology. 37 (4): 323–6. ISSN 0145-6296. PMID 8540219.
- Neumann CM, Giffin S, Hall R, Henderson M, Buhler DR (1 January 2000). "Oregon's Toxic Household Products Law". Journal of Public Health Policy. 21 (3): 342–59. doi:10.2307/3343331. ISSN 0197-5897. JSTOR 3343331. PMID 11021047. S2CID 26021475.
- Saunders, Morgan (June 2, 2009). "Law Targets Poisonings by Antifreeze". groundreport.com. Archived from the original on June 7, 2009. Retrieved 2009-06-18.
- Mullins ME, Zane Horowitz B (June 2004). "Was it necessary to add Bitrex (denatonium benzoate) to automotive products?". Veterinary and Human Toxicology. 46 (3): 150–2. ISSN 0145-6296. PMID 15171494.
- White NC, Litovitz T, Benson BE, Horowitz BZ, Marr-Lyon L, White MK (November 2009). "The impact of bittering agents on pediatric ingestions of antifreeze". Clinical Pediatrics. 48 (9): 913–21. doi:10.1177/0009922809339522. PMID 19571333. S2CID 25371911.
- Foley Peter; et al. (2002). "Ethylene glycol toxicosis in a free-ranging raccoon (Procyon lotor) from Prince Edward Island". The Canadian Veterinary Journal. 43 (4): 291–292. PMC 339239. PMID 11963664.
- "The Merck Veterinary Manual: Overview of Ethylene Glycol Toxicity" Archived 2017-01-18 at the Wayback Machine, accessed Sept. 11, 2014.
- Hanzlik PJ, Seidenfeld MA, Johnson CC (1931). "General properties, irritant and toxic actions of ethylene glycol". The Journal of Pharmacology and Experimental Therapeutics. 41 (4): 387–406. Archived from the original on 2008-10-13.
- "Concise International Chemical Assessment Document 22: Ethylene Glycol: Environmental Aspects" Archived 2013-10-31 at the Wayback Machine, World Health Organization, 2000.
- "Preliminary Data Summary: Airport Deicing Operations (Revised)" Archived 2014-03-27 at the Wayback Machine, United States Environmental Protection Agency, August 2000.
- "Glycol Guidelines" Archived 2014-09-13 at the Wayback Machine, Government of Canada, Environment Canada, Jan. 20, 1994.
- "Glycol Mitigation Strategies: The Canadian Approach" Archived 2014-09-13 at the Wayback Machine, Saleem Sattar, Transport Canada, Sept. 26, 2007.
- "Airport Deicing Effluent Guidelines" Archived 2015-02-21 at the Wayback Machine, United States Environmental Protection Agency, accessed Sept. 12, 2014.
- ANTIFREEZE POISONING… VODKA AS AN ANTIDOTE?. Pet Poison Helpline.
External links
- "Antifreeze Poisoning in Dogs & Cats (Ethylene Glycol Poisoning)" – Pet Poison Helpline
- "Antifreeze Poisoning" – Washington State University, College of Veterinary Medicine information sheet
- "Overview of Ethylene Glycol Toxicity" – Merck Veterinary Manual information.
| Inorganic |
| ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Organic |
| ||||||||||||
| Pharmaceutical |
| ||||||||||||
| Biological2 |
| ||||||||||||
| Miscellaneous | |||||||||||||
| |||||||||||||