Epidemiology of schizophrenia
Schizophrenia affects around 0.3–0.7% of people at some point in their life,[1] or 21 million people worldwide as of 2020 (about one of every 285).[2] By using precise methods in its diagnosis and a large, representative population, schizophrenia seems to occur with relative consistency over time during the last half-century.[3]
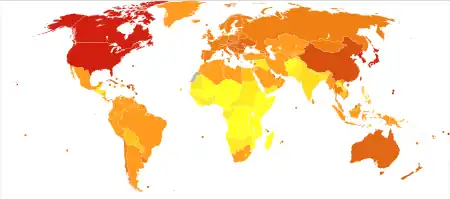
While it is claimed that schizophrenia occurs at similar rates worldwide, its prevalence and incidence varies across the world,[4] within countries,[5] and at the local and neighborhood level.[6] It causes approximately 1% of worldwide disability-adjusted life years (DALYs).[7] The rate of schizophrenia varies up to threefold depending on how it is defined.[1]
By age and gender
Schizophrenia is diagnosed 1.4 times more frequently in males than females, and typically appears earlier in men[7]—the peak ages of onset are 20–28 years for males and 26–32 years for females.[8] Onset in childhood, before the age of 13 can sometimes occur.[9][10] A later onset can occur between the ages of 40 and 60, known as late onset, and also after 60 known as very late onset.[11]
Generally, the mean age of first hospital admission for treatment of schizophrenia is between 25 and 35. Studies have suggested that lower income individuals tend to have their disorder diagnosed later after the onset of symptoms, relative to those of better economic standings. As a result, the lower social classes are more likely to be living with their illness untreated.[3]
It is generally accepted that women tend to present with schizophrenia anywhere between 4–10 years after their male counterparts.[12] However, using broad criteria for diagnosing schizophrenia shows that males have a bimodal age of onset, with peaks at 21.4 years and 39.2 years old, while females have a trimodal age of onset with peaks at 22.4, 36.6, and 61.5 years old.[13]
This additional post-menopausal peak of late-onset schizophrenia in women calls into question the etiology of the disease and raises a debate about "subtypes" of schizophrenia, with men and women being susceptible to different types (see causes of schizophrenia). This is further supported by the variability in presentation of the disease between the genders.[14]
Other theories that may explain this difference include protective or predisposing factors in men or women that may render them more (or less) susceptible to the disease at different points in life. For example, estrogen may be a protective factor for women, as estradiol has been found to be effective in treating schizophrenia when added to antipsychotic therapy.[14]
By country
In 2000, the World Health Organization found the prevalence and incidence of schizophrenia to be roughly similar around the world, with age-standardized prevalence per 100,000 ranging from 343 in Africa to 544 in Japan and Oceania for men and from 378 in Africa to 527 in Southeastern Europe for women.[15]
However, the impact of schizophrenia tends to be highest in Oceania, the Middle East, and East Asia, while the nations of Australia, Japan, the United States, and most of Europe typically have low impact. Despite relative geographical proximity, the DALY rate of schizophrenia in Indonesia is nearly double that of Australia (the nations with the highest and lowest respective DALY rates). Discrepancies between DALY rates and prevalence may arise from differences in availability of medical treatment: years lived with mental disorders carry significantly higher DALY values when unmedicated than when medicated.[15]
United States
In 2010, there were approximately 397,200 hospitalizations for schizophrenia in the United States. About 88,600 (22.3%) were readmitted within 30 days.[16]
By race
In Western Europe it has been documented that immigrant groups are more likely to be diagnosed with schizophrenia. The immigrant groups that are predominate in the increased schizophrenia diagnosis are of black origin.[17] The highest rates of schizophrenia diagnosis come from those of Afro-Caribbean ethnicity and those with black African descent.[17] In the US, African Americans have been found to be three times more likely to be diagnosed with schizophrenia, and when taking socioeconomic status into account they are two times more likely than their white counterparts.[17] However, those diagnosed with schizophrenia in developing countries have been found to have better course and outcome than their counterparts in industrialized countries.[18] These improved outcomes may be because these countries place emphasis on harmonious interpersonal relationships.[18]
Prenatal care
In two natural experiments conducted on populations that experienced famine, the rates of schizophrenia diagnosed were observed. During both the Chinese Famine (1950s) and the Dutch Hunger Winter (1944-1945) the cohorts of the exposed group were twice as likely to develop schizophrenia as compared to the unexposed cohorts.[19] It is possible that prenatal nutritional deficiency plays a role in the development of schizophrenia, in particular the lack of micronutrients. Countries with poor prenatal care, low food supply, or developing countries could have a higher incidence of schizophrenia, but more research is needed to confirm this hypothesis.
Season of Birth
This disease has been found to be correlated with the season of birth. It's known that individuals with the disease are more likely to born in the winter months. Though the risk is small, persons born in the winter months are about 10% more likely to develop schizophrenia. [20]
Cannabis Use
There have been several studies done that show a connection between schizophrenia and cannabis. The genetic liability for people with cannabis use disorder was strongly correlated to schizophrenia. It was also found to show mixed evidence that pointed to an occasional connection between cannabis use disorder and schizophrenia.[21]
References
- van Os J, Kapur S (August 2009). "Schizophrenia". Lancet. 374 (9690): 635–645. doi:10.1016/S0140-6736(09)60995-8. PMID 19700006. S2CID 208792724.
- "Schizophrenia". World Health Organization. 2011. Retrieved February 27, 2011.
- Häfner H, an der Heiden W (March 1997). "Epidemiology of schizophrenia". Canadian Journal of Psychiatry. 182 (2): 139–151. doi:10.1177/070674379704200204. PMID 9067063. S2CID 24401109.
- Jablensky A, Sartorius N, Ernberg G, Anker M, Korten A, Cooper JE, et al. (1992). "Schizophrenia: manifestations, incidence and course in different cultures. A World Health Organization ten-country study". Psychological Medicine. Monograph Supplement. 20: 1–97. doi:10.1017/S0264180100000904. PMID 1565705. S2CID 44841074.
- Kirkbride JB, Fearon P, Morgan C, Dazzan P, Morgan K, Tarrant J, et al. (March 2006). "Heterogeneity in incidence rates of schizophrenia and other psychotic syndromes: findings from the 3-center AeSOP study". Archives of General Psychiatry. 63 (3): 250–258. doi:10.1001/archpsyc.63.3.250. PMID 16520429.
- Kirkbride JB, Fearon P, Morgan C, Dazzan P, Morgan K, Murray RM, Jones PB (June 2007). "Neighbourhood variation in the incidence of psychotic disorders in Southeast London". Social Psychiatry and Psychiatric Epidemiology. 42 (6): 4998–445. doi:10.1007/s00127-007-0193-0. PMID 17473901. S2CID 19655724.
- Picchioni MM, Murray RM (July 2007). "Schizophrenia". BMJ. 335 (7610): 91–95. doi:10.1136/bmj.39227.616447.BE. PMC 1914490. PMID 17626963.
- Castle D, Wessely S, Der G, Murray RM (December 1991). "The incidence of operationally defined schizophrenia in Camberwell, 1965-84". The British Journal of Psychiatry. 159 (6): 790–794. doi:10.1192/bjp.159.6.790. PMID 1790446. S2CID 41661565.
- Diagnostic and statistical manual of mental disorders : DSM-5 (5th ed.). American Psychiatric Association. 2013. pp. 99-105. ISBN 978-0-89042-555-8.
- Da Fonseca D, Fourneret P (December 2018). "[Very early onset schizophrenia]". L'Encéphale. 44 (6S): S8–S11. doi:10.1016/S0013-7006(19)30071-5. PMID 30935493. S2CID 150798223.
- Murante T, Cohen CI (January 2017). "Cognitive Functioning in Older Adults With Schizophrenia". Focus. 15 (1): 26–34. doi:10.1176/appi.focus.20160032. PMC 6519630. PMID 31975837.
- Häfner H, Maurer K, Löffler W, Fätkenheuer B, an der Heiden W, Riecher-Rössler A, et al. (April 1994). "The epidemiology of early schizophrenia. Influence of age and gender on onset and early course". The British Journal of Psychiatry. Supplement. 164 (23): 29–38. doi:10.1192/S0007125000292714. PMID 8037899. S2CID 39681522.
- Castle D, Sham P, Murray R (October 1998). "Differences in distribution of ages of onset in males and females with schizophrenia". Schizophrenia Research. 33 (3): 179–183. doi:10.1016/s0920-9964(98)00070-x. PMID 9789910. S2CID 22355423.
- Kulkarni J, Riedel A, de Castella AR, Fitzgerald PB, Rolfe TJ, Taffe J, Burger H (March 2001). "Estrogen - a potential treatment for schizophrenia". Schizophrenia Research. 48 (1): 137–144. doi:10.1016/s0920-9964(00)00088-8. PMID 11278160. S2CID 42146691.
- Ayuso-Mateos JL. "Global burden of schizophrenia in the year 2000" (PDF). World Health Organization. Retrieved February 27, 2013.
- Elixhauser A, Steiner C. Readmissions to U.S. Hospitals by Diagnosis, 2010. HCUP Statistical Brief #153. Agency for Healthcare Research and Quality. April 2013.
- Bresnahan M, Begg MD, Brown A, Schaefer C, Sohler N, Insel B, et al. (August 2007). "Race and risk of schizophrenia in a US birth cohort: another example of health disparity?". International Journal of Epidemiology. 36 (4): 751–758. doi:10.1093/ije/dym041. PMID 17440031.
- Bae SW, Brekke JS (2002-01-01). "Characteristics of Korean-Americans with schizophrenia: a cross-ethnic comparison with African-Americans, Latinos, and Euro-Americans". Schizophrenia Bulletin. 28 (4): 703–717. doi:10.1093/oxfordjournals.schbul.a006974. PMID 12795500.
- Brown AS, Susser ES (November 2008). "Prenatal nutritional deficiency and risk of adult schizophrenia". Schizophrenia Bulletin. 34 (6): 1054–1063. doi:10.1093/schbul/sbn096. PMC 2632499. PMID 18682377.
- Messias, Erick L.; Chen, Chuan-Yu; Eaton, William W. (September 2007). "Epidemiology of Schizophrenia: Review of Findings and Myths". Psychiatric Clinics of North America. 30 (3): 323–338. doi:10.1016/j.psc.2007.04.007. ISSN 0193-953X. PMC 2727721. PMID 17720026.
- Johnson EC, Hatoum AS, Deak JD, Polimanti R, Murray RM, Edenberg HJ, et al. (November 2021). "The relationship between cannabis and schizophrenia: a genetically informed perspective". Addiction. 116 (11): 3227–3234. doi:10.1111/add.15534. PMC 8492483. PMID 33950550.
Further reading
- Saha S, Chant D, Welham J, McGrath J (May 2005). "A systematic review of the prevalence of schizophrenia". PLOS Medicine. 2 (5): e141. doi:10.1371/journal.pmed.0020141. PMC 1140952. PMID 15916472.