Cocaine dependence
Cocaine dependence is a neurological disorder that is characterized by withdrawal symptoms upon cessation from cocaine use.[1] It also often coincides with cocaine addiction which is a biopsychosocial disorder characterized by persistent use of cocaine and/or crack despite substantial harm and adverse consequences. The Diagnostic and Statistical Manual of Mental Disorders (5th ed., abbreviated DSM-5), classifies problematic cocaine use as a "Stimulant use disorder".[2] The International Classification of Diseases (11th rev., abbreviated ICD-11), includes "Cocaine dependence" as a classification (diagnosis) under "Disorders due to use of cocaine".[3]
| Cocaine dependence | |
|---|---|
| Specialty | Psychiatry, clinical psychology |
The use of cocaine creates euphoria and high amounts of energy. If taken in large doses, it is possible to cause mood swings, paranoia, insomnia, psychosis, high blood pressure, a fast heart rate, panic attacks, seizures that are extremely difficult to control, cognitive impairments and drastic changes in personality. Cocaine overdose may result in cardiovascular and brain damage, such as: status epilepticus, constricting blood vessels in the brain, causing strokes and constricting arteries in the heart; causing heart attacks.[4]
The symptoms of cocaine withdrawal range from moderate to severe: dysphoria, depression, anxiety, decreased libido, psychological and physical weakness, pain, and compulsive cravings.
Signs and symptoms
Cocaine is a powerful stimulant known to make users feel energetic, cheerful, talkative, etc. In time, negative side effects include increased body temperature, irregular or rapid heart rate, high blood pressure, increased risk of heart attacks, strokes and even sudden death from cardiac arrest.[5] Many people who habitually use cocaine develop a transient, manic-like condition similar to amphetamine psychosis and schizophrenia, whose symptoms include aggression, severe paranoia, restlessness, confusion[6] and tactile hallucinations; which can include the feeling of something crawling under the skin (formication), also known as "coke bugs", during binges.[7] Different ingestion techniques have their own symptoms that accompany them. Snorting it can cause a loss of sense of smell, nose bleeds, problems swallowing and an inflamed, runny nose. Smoking it causes lung damage and injecting it puts users at risk of contracting infectious diseases like HIV and hepatitis C[8]. Heavy users of cocaine have also reported having thoughts of suicide, unusual weight loss, trouble maintaining relationships, and an unhealthy, pale appearance.[6]
Withdrawal symptoms
When used habitually, cocaine, because of its highly addictive nature, can change brain structure and function.[8] Circuits within the brain structure that play a part in stress signals become more sensitive. When cocaine is not being used this increases an individual's displeasure and negative moods.[8] In 1986, Gawin and Kleber led an important study on the withdrawal symptoms of cocaine users. In this study, three distinct phases were reported. These phases are the 'crash', 'withdrawal' and 'extinction'.[9] The 'crash' phase or phase 1 occurs directly after cocaine is not being used anymore. Withdrawal symptoms for this phase are exhaustion, hypersomnia, no cravings to use, dysthymia, increased appetite, restlessness, and irritability.[9] The second phase, or 'withdrawal' phase occurs 1–10 weeks after cocaine users quit, symptoms include: lethargy, anxiety, erratic sleep, strong craving, emotional lability, irritability, depression, poor concentration, and bowel issues.[9] Finally the last phase or the 'extinction' phase occurs up to 28 weeks after discontinued use, symptoms include: episodic cravings and some dysphoria.[9]
Epidemiology and prevalence rates
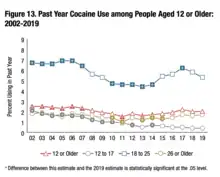
In the United States, past year cocaine users in 2019 was 5.5 million for people aged 12 or older. When broken into age groups, ages 12–17 had 97,000 users; ages 18–25 had 1.8 million users and ages 26 or older had 3.6 million users.[10]
Past year cocaine users with a cocaine use disorder in 2019 was 1 million for people aged 12 or older. When broken into age groups, ages 12–17 had 5,000 people with a cocaine use disorder; ages 18–25 had 250,000 people with a cocaine use disorder and ages 26 or older had 756,000 people with a cocaine use disorder[10]
In the United States, cocaine use overdose deaths have been on the rise and in 2019, the CDC reported over 16,000 deaths from cocaine overdose.[11]
Risk
A study consisting of 1,081 U.S. residents who had first used cocaine within the previous 24 months was conducted. It was found that the risk of becoming dependent on cocaine within two years of first use was 5–6%. The risk of becoming dependent within 10 years of first use increased to 15–16%. These were the aggregate rates for all types of use considered, such as smoking, snorting, and injecting. Among recent-onset users individual rates of dependency were higher for smoking (3.4 times) and much higher for injecting. Women were 3.3 times more likely to become dependent, compared with men. Users who started at ages 12 or 13 were four times as likely to become dependent compared to those who started between ages 18 and 20.[12][13][14]
However, a study of non-deviant[nb 1] users in Amsterdam found a "relative absence of destructive and compulsive use patterns over a ten year period" and concluded that cocaine users can and do exercise control. "Our respondents applied two basic types of controls to themselves: 1) restricting use to certain situations and to emotional states in which cocaine's effects would be most positive, and 2) limiting mode of ingestion to snorting of modest amounts of cocaine, staying below 2.5 grams a week for some, and below 0.5 grams a week for most. Nevertheless, those whose use level exceeded 2.5 grams a week all returned to lower levels".[15]
Treatment
Therapy
Twelve-step programs such as Cocaine Anonymous (modeled on Alcoholics Anonymous) have been widely used to help those with cocaine addiction. Cognitive behavioral therapy (CBT), dialectical behavior therapy (DBT), rational emotive behavior therapy (REBT), and motivational interviewing (MI) can be especially powerful approaches to treating cocaine addiction.[16] Cognitive behavioral therapy (CBT) combined with motivational therapy (MT) have proven to be more helpful than 12 step programs in treating cocaine dependency.[17] However, both these approaches have a fairly low success rate as research suggests that the withdrawal symptoms can last for several weeks.[18][19][20] For instance, one of the main predictors of a successful recovery is dependent on the number of continuous days a user is able to stay off of the substance.[18][21] Alternative holistic treatments such as physical exercise and Meditation has been proven effective in reducing cocaine cravings.[4] Other non-pharmacological treatments such as acupuncture[22][23] and hypnosis have been explored, but without conclusive results.[24][25]
Medications
Numerous medications have been investigated for use in cocaine dependence, but as of 2015, none of them were considered to be effective.[26] Anticonvulsants, such as carbamazepine, gabapentin, lamotrigine, and topiramate, do not appear to be effective as treatment.[26][27] Limited evidence suggests that antipsychotics are also ineffective for treatment of cocaine dependence.[28] Few studies have examined bupropion (a novel antidepressant) for cocaine dependence; however, trials performed thus far have not shown it to be an effective form of treatment for this purpose.[29]
The National Institute on Drug Abuse (NIDA) of the U.S. National Institutes of Health is researching modafinil, a narcolepsy drug and mild stimulant, as a potential cocaine treatment. Ibogaine has been under investigation as a treatment for cocaine dependency and is used in clinics in Mexico, the Netherlands and Canada. It was legal for a time in Costa Rica, but has been illegal since 2018. It is illegal to use in many countries, such as Sweden, Norway, the United Kingdom, and in the United States.[30] Other medications that have been investigated for this purpose include acetylcysteine, baclofen,[31] and vanoxerine.[32] Medications such as phenelzine, have been used to cause an "aversion reaction" when administered with cocaine.[lower-alpha 1]
Research
Transcranial magnetic stimulation (TMS) is being studied as a treatment for cocaine addiction, although definitive evidence for efficacy does not yet exist.[35][36]
Other research on rodents has suggested that cocaine use leads to complexes of dopamine transporters, which build up tolerance to the drug.[37] It's possible that future treatment for cocaine addiction might target those complexes.[37][38]
See also
- SB-277011-A – a dopamine D3 receptor antagonist, used in the study of cocaine addiction. Where cocaine reduces the threshold for brain electrical self-stimulation in rats, an indication of cocaine's rewarding effects, SB-277011-A completely reverses this effect.
Notes
- The study's authors stated that they wanted to know which effects and consequences of cocaine use would become visible with persons who are mainstream citizens or as close to that social stratum as possible
References
- Pomara C, Cassano T, D'Errico S, Bello S, Romano AD, Riezzo I, Serviddio G (2012). "Data available on the extent of cocaine use and dependence: biochemistry, pharmacologic effects and global burden of disease of cocaine abusers". Current Medicinal Chemistry. 19 (33): 5647–57. doi:10.2174/092986712803988811. PMID 22856655.
- Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Arlington, VA: American Psychiatric Association Publishing. 2013. p. 561. ISBN 978-089042-555-8.
- "6C45 Disorders due to use of cocaine". ICD-11 - Mortality and Morbidity Statistics. Retrieved 20 November 2020.
- Cocaine Use and Its Effects
- Walsh, Karen (October 2010). "Teen Cocaine Use". Inspirations for Youth and Family. Archived from the original on 13 February 2018. Retrieved 12 December 2013.
- LeVert, Suzanne (2006). Drugs: The Facts About Cocaine. New York: Marshall Cavendish Benchmark. pp. 41, 76.
- Gawin, F.H. (1991). "Cocaine addiction: Psychology and neurophysiology". Science. 251 (5001): 1580–6. Bibcode:1991Sci...251.1580G. doi:10.1126/science.2011738. PMID 2011738. S2CID 26660048.
- Abuse, National Institute on Drug. "What is Cocaine?". National Institute on Drug Abuse. Retrieved 9 May 2021.
- "Department of Health | The cocaine withdrawal syndrome". www1.health.gov.au. Retrieved 10 May 2021.
- "National Survey on Drug Use and Health". nsduhweb.rti.org. Retrieved 9 May 2021.
- Abuse, National Institute on Drug. "Cocaine". National Institute on Drug Abuse. Retrieved 1 May 2021.
- Tierney, John (16 September 2013). "The Rational Choices of Crack Addicts". New York Times. Retrieved 16 September 2013.
- Wagner, FA (2002), "From first drug use to drug dependence; developmental periods of risk for dependence upon marijuana, cocaine, and alcohol", Neuropsychopharmacology, 26 (4): 479–88, doi:10.1016/S0893-133X(01)00367-0, PMID 11927172
- O'Brien MS, Anthony JC (2005). "Risk of becoming cocaine dependent: epidemiological estimates for the United States, 2000–2001". Neuropsychopharmacology. 30 (5): 1006–1018. doi:10.1038/sj.npp.1300681. PMID 15785780.
- Cohen, Peter; Sas, Arjan (1994). "Cocaine use in Amsterdam in non deviant subcultures". Addiction Research. 2 (1): 71–94. doi:10.3109/16066359409005547.
- "Cocaine and Addiction". Niznik Behaviour Health.
- Palinkas, L. A. (17 January 2008). "Cognitive behavioural therapy reduced cocaine abuse compared with 12 step facilitation". Evidence-Based Mental Health. ebmh.bmj.com. 2 (2): 51. doi:10.1136/ebmh.2.2.51. S2CID 146360156. Retrieved 25 August 2012.
- Barbee, Britton R.; Gourley, Shannon L. (1 June 2022). "Brain systems in cocaine abstinence-induced anxiety-like behavior in rodents: A review". Addiction Neuroscience. 2: 100012. doi:10.1016/j.addicn.2022.100012. ISSN 2772-3925. PMC 10361393. PMID 37485439. S2CID 247587106.
- Gawin, Frank H. (1 February 1986). "Abstinence Symptomatology and Psychiatric Diagnosis in Cocaine Abusers: Clinical Observations". Archives of General Psychiatry. 43 (2): 107–113. doi:10.1001/archpsyc.1986.01800020013003. ISSN 0003-990X. PMID 3947206.
- McHugh, R. Kathryn; Hearon, Bridget A.; Otto, Michael W. (September 2010). "Cognitive-Behavioral Therapy for Substance Use Disorders". Psychiatric Clinics of North America. 33 (3): 511–525. doi:10.1016/j.psc.2010.04.012. PMC 2897895. PMID 20599130.
- Carroll, Kathleen M.; Kiluk, Brian D.; Nich, Charla; DeVito, Elise E.; Decker, Suzanne; LaPaglia, Donna; Duffey, Dianne; Babuscio, Theresa A.; Ball, Samuel A. (1 April 2014). "Toward empirical identification of a clinically meaningful indicator of treatment outcome: Features of candidate indicators and evaluation of sensitivity to treatment effects and relationship to one year follow up cocaine use outcomes". Drug and Alcohol Dependence. 137: 3–19. doi:10.1016/j.drugalcdep.2014.01.012. ISSN 0376-8716. PMC 4042667. PMID 24556275.
- Margolin, Arthur; et al. (2 January 2002). "Acupuncture for the treatment of cocaine addiction: A randomized controlled trial". The Journal of the American Medical Association. 287 (1): 55–63. doi:10.1001/jama.287.1.55. PMID 11754709.
- Otto, Katharine C.; Quinn, Colin; Sung, Yung-Fong (Spring 1998). "Auricular acupuncture as an adjunctive treatment for cocaine addiction: A pilot study". The American Journal on Addictions. 7 (2): 164–170. doi:10.1111/j.1521-0391.1998.tb00331.x. PMID 9598220.
- Page, R.A.; Handleya, G.W. (1993). "The use of hypnosis in cocaine addiction". American Journal of Clinical Hypnosis. 36 (2): 120–123. doi:10.1080/00029157.1993.10403054. PMID 8259763.
- Potter, Greg (2004). "Intensive therapy: Utilizing hypnosis in the treatment of substance abuse disorders". American Journal of Clinical Hypnosis. 47 (1): 21–28. doi:10.1080/00029157.2004.10401472. PMID 15376606. S2CID 42943267.
- Minozzi, S; Cinquini, M; Amato, L; Davoli, M; Farrell, MF; Pani, PP; Vecchi, S (April 2015). "Anticonvulsants for cocaine dependence". Cochrane Database of Systematic Reviews (Systematic Review & Meta-Analysis). 17 (4): CD006754. doi:10.1002/14651858.CD006754.pub4. PMC 8812341. PMID 25882271.
- Singh, M; Keer, D; Klimas, J; Wood, E; Werb, D (August 2016). "Topiramate for cocaine dependence: a systematic review and meta-analysis of randomized controlled trials". Addiction (Systematic Review & Meta-Analysis). 111 (8): 1337–46. doi:10.1111/add.13328. hdl:10147/596595. PMID 26826006. S2CID 34637139.
- Indave, BI; Minozzi, S; Pani, PP; Amato, L (March 2016). "Antipsychotic medications for cocaine dependence". Cochrane Database of Systematic Reviews (Systematic Review and Meta-Analysis). 3 (6): CD006306. doi:10.1002/14651858.CD006306.pub3. PMC 8750745. PMID 26992929.
- Mariani, JJ; Levin, FR (June 2012). "Psychostimulant treatment of cocaine dependence". Psychiatric Clinics of North America (Review). 35 (2): 425–39. doi:10.1016/j.psc.2012.03.012. PMC 3417072. PMID 22640764.
- Group, Clear Sky (1 August 2018). "Is Ibogaine Illegal in the United States?". Clear Sky Recovery. Retrieved 6 May 2021.
- Karila L; Gorelick D; Weinstein A; et al. (May 2008). "New treatments for cocaine dependence: a focused review". Int. J. Neuropsychopharmacol. 11 (3): 425–38. doi:10.1017/S1461145707008097. PMID 17927843.
- Cherstniakova SA, Bi D, Fuller DR, Mojsiak JZ, Collins JM, Cantilena LR (September 2001). "Metabolism of vanoxerine, 1-[2-[bis(4-fluorophenyl)methoxy]ethyl]-4-(3-phenylpropyl)piperazine, by human cytochrome P450 enzymes". Drug Metab. Dispos. 29 (9): 1216–20. PMID 11502731.
- "Chemistry, Design, and Structure-Activity Relationship of Cocaine Antagonists". Satendra Singh et al. Chem. Rev. 2000, 100. 925-1024. PubMed; Chemical Reviews (Impact Factor: 45.66). 04/2000; 100(3):925-1024 American Chemical Society; 2000, ISSN 0009-2665 ChemInform; May, 16th 2000, Volume 31, Issue 20, DOI: 10.1002/chin.200020238. Mirror hotlink.
- Martell BA, Mitchell E, Poling J, Gonsai K, Kosten TR (July 2005). "Vaccine pharmacotherapy for the treatment of cocaine dependence". Biol. Psychiatry. 58 (2): 158–64. doi:10.1016/j.biopsych.2005.04.032. PMID 16038686. S2CID 22415520.
- Wadman, Meredith (29 August 2017). "Brain-altering magnetic pulses could zap cocaine addiction". Science Magazine. American Association for the Advancement of Science. Retrieved 1 September 2017.
- Rachid, Fady (1 January 2018). "Neurostimulation techniques in the treatment of cocaine dependence: A review of the literature". Addictive Behaviors. 76: 145–155. doi:10.1016/j.addbeh.2017.08.004. ISSN 0306-4603. PMID 28822321.
- Siciliano, Cody A.; Saha, Kaustuv; Calipari, Erin S.; Fordahl, Steve C.; Chen, Rong; Khoshbouei, Habibeh; Jones, Sara R. (10 January 2018). "Amphetamine Reverses Escalated Cocaine Intake via Restoration of Dopamine Transporter Conformation". The Journal of Neuroscience. 38 (2): 484–497. doi:10.1523/JNEUROSCI.2604-17.2017. ISSN 1529-2401. PMC 5761621. PMID 29175958.
- "Cocaine Addiction Treatment".
Reference notes
- [33] ←Page #928 (4th page of article) ¶4. §(1), (2) & (3); Lines 10—12 & 15—18 of aforementioned 4th ¶.
External links
| Addiction |
| ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dependence |
| ||||||||||
| Treatment and management |
| ||||||||||
| See also |
| ||||||||||
| |||||||||||
| General |  | ||||
|---|---|---|---|---|---|
| Combined substance use |
| ||||
| Alcohol |
| ||||
| Caffeine | |||||
| Cannabis |
| ||||
| Cocaine |
| ||||
| Hallucinogen | |||||
| Nicotine | |||||
| Opioids |
| ||||
| Sedative / hypnotic | |||||
| Stimulants | |||||
| Volatile solvent |
| ||||
| Related | |||||