Arcuate uterus
The arcuate uterus is a form of a uterine anomaly or variation where the uterine cavity displays a concave contour towards the fundus. Normally the uterine cavity is straight or convex towards the fundus on anterior-posterior imaging, but in the arcuate uterus the myometrium of the fundus dips into the cavity and may form a small septation. The distinction between an arcuate uterus and a septate uterus is not standardized.
| Arcuate uterus | |
|---|---|
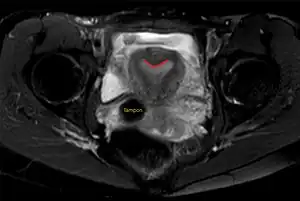 | |
| Arcuate uterus (marked in red) seen on MRI | |
| Specialty | Gynaecology |
Signs and symptoms
The condition may not be known to the affected individual and not result in any reproductive problems; thus normal pregnancies occur.[1] Indeed, there is no consensus on the relationship of the arcuate uterus and recurrent pregnancy loss.[2] Accordingly, the condition may be a variation or a pathology.
One view maintains that the condition is associated with a higher risk for miscarriage, premature birth, and malpresentation. Thus a study that evaluated women with uterine bleeding by hysteroscopy found that 6.5% of subjects displayed the arcuate uterus and had evidence of reproductive impairments.[3] A study based on hysterosalpingraphic detected arcuate lesions documented increased fetal loss and obstetrical complications as a risk for affected women.[4] Woelfer found that the miscarriage risk is more pronounced in the second trimester.[5] In contrast, a study utilizing 3-D ultrasonography to document the prevalence of the arcuate uterus in a gynecological population found no evidence of increased risk of reproductive loss; in this study 3.1% of women had an arcuate uterus making it the most common uterine anomaly; this prevalence was similar than in women undergoing sterilization and lower than in women with recurrent pregnancy loss.[6]
Cause
The uterus is formed during embryogenesis by the fusion of the two Müllerian ducts. During this fusion a resorption process eliminates the partition between the two ducts to create a single cavity. This process begins caudally and advances cranially, thus an arcuate uterus represents an in the final stage incomplete absorption process.
Diagnosis
A transvaginal ultrasound can reveal the condition.
Helpful techniques to investigate the uterine structure are transvaginal ultrasonography and sonohysterography, hysterosalpingography, MRI, and hysteroscopy. More recently 3-D ultrasonography has been advocated as an excellent non-invasive method to delineate the condition.[5]
Differential diagnosis
The major differential diagnosis is the uterine septum. The lack of agreement to separate these two entities makes it difficult to assess the results in the literature.
Management
Many patients with an arcuate uterus will not experience any reproductive problems and do not require any surgery. In patients with recurrent pregnancy loss thought to be caused by an arcuate uterus hysteroscopic resection can be performed.
Epidemiology
Most studies of uterine malformations are based on populations of women who have experienced a miscarriage and thus do not address the issue of the prevalence in the general population. A screening study by Woelfer et al. of women without a history of reproductive problems found that about 5% of women had an arcuate uterus when they defined an arcuate uterus any fundal protrusion into the cavity that had an apical angle of more than 90 degrees. Accordingly, it was the most common uterine anomaly, followed by septate uterus (3%) and bicornuate uterus (0.5%).[5]
References
- Creasy RK, Resnik R (1994). Maternal-Fetal Medicine: Principles and Practice. Philadelphia: W.B. Saunders. p. 447. ISBN 978-0-7216-6590-0.
- ACOG (2001). "Management of Recurrent Early Pregnancy Loss". Practice Bulletin (24): 3.
- Maneschi F, Zupi E, Marconi D, Valli E, Romanini C, Mancuso S (1995). "Hysteroscopically detected asymptomatic müllerian anomalies. Prevalence and reproductive implications". J Reprod Med. 40 (10): 684–8. PMID 8551467.
- Sørensen SS, Trauelsen AG (1987). "Obstetric implications of minor müllerian anomalies in oligomenorrheic women". Am. J. Obstet. Gynecol. 156 (5): 1112–8. doi:10.1016/0002-9378(87)90121-9. PMID 3578421.
- Woelfer B, Salim R, Banerjee S, Elson J, Regan L, Jurkovic D (2001). "Reproductive outcomes in women with congenital uterine anomalies detected by three-dimensional ultrasound screening (by Google Scholar search)". Obstet Gynecol. 98 (6): 1099–103. doi:10.1016/S0029-7844(01)01599-X. PMID 11755560. S2CID 37650526.
- Jurkovic D, Gruboeck K, Tailor A, Nicolaides KH (1997). "Ultrasound screening for congenital uterine anomalies". Br J Obstet Gynaecol. 104 (11): 1320–1. doi:10.1111/j.1471-0528.1997.tb10982.x. PMID 9386036. S2CID 6316625.