Underweight
An underweight person is a person whose body weight is considered too low to be healthy. A person who is underweight is malnourished.
| Underweight | |
|---|---|
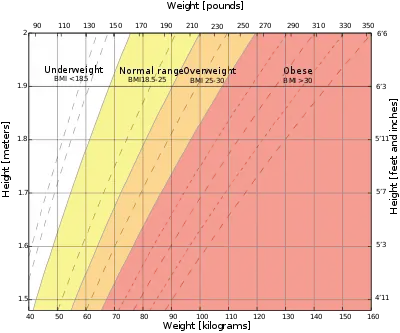 | |
| The underweight range according to the body mass index (BMI) is the white area on the chart. | |
| Specialty | Endocrinology |
| Part of a series on |
| Human body weight |
|---|
Assessment
| Category[1] | BMI (kgm−2) |
|---|---|
| Underweight (severe) | < 16.0 |
| Underweight (moderate) | 16.0 – 16.9 |
| Underweight (mild) | 17.0 – 18.4 |
| Normal weight | 18.5 – 24.9 |
| Overweight | 25.0 – 29.9 |
| Obese | ≥ 30.0 |
The body mass index, a ratio of a person's weight to their height, has traditionally been used to assess the health of a person as it pertains to weight: under the cut-off point at a BMI of 18.5, a person is considered underweight.[2] The calculation is either weight in kilograms divided by height in meters, squared, or weight in pounds times 703, divided by height in inches, squared. Another measure of underweight is through comparison to the average weight of a cohort of people of a similar age and height: people who are at least 15% to 20% below the average weight for the group are considered underweight.[3]
Body fat percentage has been suggested as another way to assess whether a person is underweight. Unlike the body mass index, which is a proxy measurement, the body fat percentage takes into account the difference in composition between adipose tissue (fat cells) and muscle tissue and their different roles in the body.[4] The American Council on Exercise defines the amount of essential fat, below which a person is underweight, as 10–13% for women and 2–5% for men.[5] The greater amount of essential body fat in women supports reproductive function.
Prevalence
Using the body mass index as a measure of weight-related health, with data from 2014, age-standardised global prevalence of underweight in women and men were 9.7% and 8.8%, respectively. These values were lower than what was reported for 1975 as 14.6% and 13.8%, respectively, indicating a worldwide reduction in the extent of undernutrition.[6]
Causes
A person may be underweight due to genetics,[7][8] poor absorption of nutrients, increased metabolic rate or energy expenditure, lack of food (frequently due to poverty), drugs that affect appetite, illness (physical or mental) or the eating disorder anorexia nervosa.[9][10]
Being underweight is associated with certain medical conditions, including type 1 diabetes,[11] hyperthyroidism,[12] cancer,[13] and tuberculosis.[14] People with gastrointestinal or liver problems may be unable to absorb nutrients adequately. People with certain eating disorders can also be underweight due to one or more nutrient deficiencies or excessive exercise, which exacerbates nutrient deficiencies.[15][16]
A common belief is that healthy underweight individuals can ‘eat what they want’ and then burn it off either by high levels of activity or elevated metabolism. It has been shown, however, that individuals with BMI < 18.5 eat about 12% less calories than individuals with normal BMI (21.5 to 25) and they are 23% less physically active (by accelerometry).[17]
Problems
Being underweight can be a symptom of an underlying condition, in which case it is secondary. Unexplained weight loss may require a professional medical diagnosis by a physician.[18]
Being underweight can also cause other conditions, in which case it is primary. Severely underweight individuals may have poor physical stamina and a weak immune system, leaving them open to infection. According to Robert E. Black of the Johns Hopkins School of Public Health (JHSPH), "Underweight status ... and micronutrient deficiencies also cause decreases in immune and non-immune host defenses, and should be classified as underlying causes of death if followed by infectious diseases that are the terminal associated causes."[19] People who are malnourished raise special concerns, as not only gross caloric intake may be inadequate, but also intake and absorption of other vital nutrients, especially essential amino acids and micronutrients such as vitamins and minerals.
In women, being severely underweight, as a result of an eating disorder or due to excessive strenuous exercise, can result in amenorrhea (absence of menstruation),[20] infertility or complications during pregnancy if gestational weight gain is too low.
Malnourishment can also cause anemia and hair loss.
Being underweight is an established[21] risk factor for osteoporosis, even for young people. This is seen in individuals suffering from relative energy deficiency in sport, formerly known as female athlete triad: when disordered eating or excessive exercise cause amenorrhea, hormone changes during ovulation leads to loss of bone mineral density.[22][23] After this low bone mineral density causes the first spontaneous fractures, the damage is often irreversible.
Although being underweight has been reported to increase mortality at rates comparable to that seen in morbidly obese people,[24] the effect is much less drastic when restricted to non-smokers with no history of disease,[25] suggesting that smoking and disease-related weight loss are the leading causes of the observed effect.
Treatment
Diet
Underweight individuals may be advised to gain weight by increasing calorie intake. This can be done by eating a sufficient volume of sufficiently calorie-dense foods.[26][27][28] Body weight may also be increased through the consumption of liquid nutritional supplements.[29]
Exercise
Another way for underweight people to gain weight is by exercising, since muscle hypertrophy increases body mass. Weight lifting exercises are effective in helping to improve muscle tone as well as helping with weight gain.[30] Weight lifting has also been shown to improve bone mineral density,[31] which underweight people are more likely to lack.[32]
Exercise is catabolic, which results in a brief reduction in mass. However, during recovery, anabolic overcompensation causes the muscles to grow, which results in an overall increase in mass. This can happen through an increase in muscle proteins, or through enhanced storage of glycogen in muscles. Exercise can also help stimulate the appetite of a person who is not inclined to eat.
Appetite stimulants
Certain drugs may increase appetite either as their primary effect or as a side effect. Antidepressants, such as mirtazapine or amitriptyline, and antipsychotics, particularly chlorpromazine and haloperidol, as well as tetrahydrocannabinol (found in cannabis), all present an increase in appetite as a side effect. In states where it is approved, medicinal cannabis may be prescribed for severe appetite loss, such as that caused by cancer, AIDS, or severe levels of persistent anxiety. Other drugs or supplements which may increase appetite include antihistamines (such as diphenhydramine, promethazine or cyproheptadine).[33]
See also
References
- The SuRF Report 2 (PDF). The Surveillance of Risk Factors Report Series (SuRF). World Health Organization. 2005. p. 22.
- "Assessing Your Weight and Health Risk". National Heart, Lung and Blood Institute. Retrieved 23 September 2012.
- Mahan, L. Kathleen (2000). Krause's Food, Nutrition & Diet Therapy, 10th Ed. Philadelphia: W.B. Saunders Co.
- Pasco, Julie A.; Holloway, Kara L.; Dobbins, Amelia G.; Kotowicz, Mark A.; Williams, Lana J.; Brennan, Sharon L. (23 June 2014). "Body mass index and measures of body fat for defining obesity and underweight: a cross-sectional, population-based study". BMC Obesity. 1: 9. doi:10.1186/2052-9538-1-9. PMC 4511447. PMID 26217501.
- "ACE Fit - Body Fat Percentage Calculator". Retrieved 28 February 2020.
- NCD Risk Factor Collaboration (NCD-RisC) (April 2016). "Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants". Lancet. 387 (10026): 1377–96. doi:10.1016/S0140-6736(16)30054-X. PMID 27115820.
- "Body Shape 'Is Down to Genes'". Indian Express. Retrieved October 23, 2010.
- "'Skinny Gene' Exists". Science Daily. September 5, 2007. Retrieved October 23, 2010.
- "What are Eating Disorders?". NIMH. Archived from the original on 23 May 2015. Retrieved 24 May 2015.
- Attia E (2010). "Anorexia nervosa: current status and future directions". Annual Review of Medicine. 61 (1): 425–435. doi:10.1146/annurev.med.050208.200745. PMID 19719398.
- "Unexplained Weight Loss - Reasons, Symptoms & Causes". Retrieved 2017-11-28.
- Milas, Kresimira. "Hyperthyroidism Symptoms - Signs and symptoms caused by excessive amounts of thyroid hormones". Endocrine Web. Retrieved 24 September 2012.
- "Signs and Symptoms of Cancer". American Cancer Society. Retrieved 24 September 2012.
- Hira, S. K.; H. L. Dupont; D. N. Lanjewar; Y. N. Dholakia (1998). "Severe weight loss: the predominant clinical presentation of tuberculosis in patients with HIV infection in India". National Medical Journal of India. 11 (6): 256–58. PMID 10083790.
- Fisher MM, Rosen DS, Ornstein RM, Mammel KA, Katzman DK, Rome ES, et al. (July 2014). "Characteristics of avoidant/restrictive food intake disorder in children and adolescents: a "new disorder" in DSM-5". The Journal of Adolescent Health. 55 (1): 49–52. doi:10.1016/j.jadohealth.2013.11.013. PMID 24506978.
- Latner JD, Wilson GT (September 2000). "Cognitive-behavioral therapy and nutritional counseling in the treatment of bulimia nervosa and binge eating" (PDF). Eating Behaviors. 1 (1): 3–21. CiteSeerX 10.1.1.578.4563. doi:10.1016/S1471-0153(00)00008-8. PMID 15001063.
- Hu, S.; Zhang X.; Stamatiou M.; Hambly C.; Huang Y.; Ma J.; Li Y.; Speakman J.R. (2022). "Higher than predicted resting energy expenditure and lower physical activity in healthy underweight Chinese adults". Cell Metabolism. 34 (10): 1413–1415. doi:10.1016/j.cmet.2022.05.012. PMID 35839758. S2CID 250576685.
- "Weight loss - unintentional: MedlinePlus Medical Encyclopedia". medlineplus.gov. Retrieved 2022-11-18.
- Black, Robert E.; Morris, Saul S.; Bryce, Jennifer (28 June 2003), "Where and Why are 10 Million Children Dying Every Year?", The Lancet, 361 (9376): 2226–34, doi:10.1016/S0140-6736(03)13779-8, PMID 12842379, S2CID 14509705
- "MJH Life Sciences™ | Informing Healthcare Professionals •". 10 August 2022.
- Gjesdal; Halse, JI; Eide, GE; Brun, JG; Tell, GS (2008). "Impact of lean mass and fat mass on bone mineral density: the Hordaland Health Study". Maturitas. 59 (2): 191–200. doi:10.1016/j.maturitas.2007.11.002. PMID 18221845.
- Nattiv; Agostini, R; Drinkwater, B; Yeager, KK (1994). "The female athlete triad. The inter-relatedness of disordered eating, amenorrhea, and osteoporosis". Clinics in Sports Medicine. 13 (2): 405–18. doi:10.1016/S0278-5919(20)30338-0. PMID 8013041.
- Wilson; Wolman, RL (1994). "Osteoporosis and fracture complications in an amenorrhoeic athlete". British Journal of Rheumatology. 33 (5): 480–1. doi:10.1093/rheumatology/33.5.480. PMID 8173855.
- Waaler HT. (1984). "Height, weight and mortality. The Norwegian experience". Acta Med Scand Suppl. 215 (679): 1–56. doi:10.1111/j.0954-6820.1984.tb12901.x. PMID 6585126.
- Body Weight and Mortality:What is the optimum weight for a longer life?.
- Zeratsky, Katherine (23 August 2011). "Underweight? See how to add pounds healthfully". Nutrition and healthy eating. Mayo Clinic. Retrieved 19 March 2012.
- "Gain Weight and Be Healthy". About.com. Retrieved October 23, 2010.
- "Achieving Healthy Weight Gain". Health Central. Retrieved October 23, 2010.
- "Healthy Weight Gain". Children's Hospital Boston, Center for Young Women's Health. Retrieved October 23, 2010.
- "Men's Health". Men's Health. Retrieved October 23, 2010.
- Gleeson, Peggy; Elizabeth J. Protas; Adrian D. Leblanc; Victor S. Schneider; Harlan J. Evans (February 1990). "Effects of weight lifting on bone mineral density in premenopausal women". Journal of Bone and Mineral Research. 5 (2): 153–158. doi:10.1002/jbmr.5650050208. PMID 2316403. S2CID 72034011.
- Coin, A.; G. Sergi; P. Benincà; L. Lupoli; G. Cinti; L. Ferrara; G. Benedetti; G. Tomasi; C. Pisent; G. Enzi (2000). "Bone Mineral Density and Body Composition in Underweight and Normal Elderly Subjects". Osteoporosis International. 11 (12): 1043–1050. doi:10.1007/s001980070026. PMID 11256896. S2CID 1298271.
- Homnick, Douglas N. (2005). "Long-term trial of cyproheptadine as an appetite stimulant in cystic fibrosis". Pediatric Pulmonology. 40 (3): 251–256. doi:10.1002/ppul.20265. PMID 16015665. S2CID 22837100.