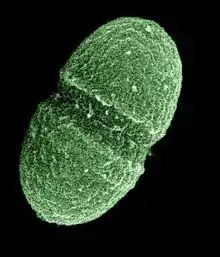
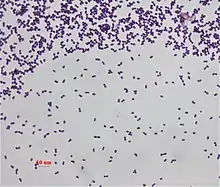
Enterococcus faecalis
Enterococcus faecalis – formerly classified as part of the group D Streptococcus system – is a Gram-positive, commensal bacterium inhabiting the gastrointestinal tracts of humans.[1][2] Like other species in the genus Enterococcus, E. faecalis is found in healthy humans and can be used as a probiotic. The probiotic strains such as Symbioflor1 and EF-2001 are characterized by the lack of specific genes related to drug resistance and pathogenesis.[3] As an opportunistic pathogen, E. faecalis can cause life-threatening infections, especially in the nosocomial (hospital) environment, where the naturally high levels of antibiotic resistance found in E. faecalis contribute to its pathogenicity.[2] E. faecalis has been frequently found in reinfected, root canal-treated teeth in prevalence values ranging from 30% to 90% of the cases.[4] Re-infected root canal-treated teeth are about nine times more likely to harbor E. faecalis than cases of primary infections.[5]
| Enterococcus faecalis | |
|---|---|
 | |
| Scientific classification | |
| Domain: | Bacteria |
| Phylum: | Bacillota |
| Class: | Bacilli |
| Order: | Lactobacillales |
| Family: | Enterococcaceae |
| Genus: | Enterococcus |
| Species: | E. faecalis |
| Binomial name | |
| Enterococcus faecalis (Andrewes and Horder, 1906) Schleifer and Kilpper-Bälz, 1984 | |
Physiology
E. faecalis is a nonmotile microbe; it ferments glucose without gas production, and does not produce a catalase reaction with hydrogen peroxide. It produces a reduction of litmus milk, but does not liquefy gelatin. It shows consistent growth throughout nutrient broth which is consistent with being a facultative anaerobe. It catabolizes a variety of energy sources, including glycerol, lactate, malate, citrate, arginine, agmatine, and many keto acids. Enterococci survive very harsh environments, including extremely alkaline pH (9.6) and salt concentrations. They resist bile salts, detergents, heavy metals, ethanol, azide, and desiccation. They can grow in the range of 10 to 45 °C and survive at temperatures of 60 °C for 30 min.[6]
Pathogenesis
E. faecalis is found in most healthy individuals, but can cause endocarditis and sepsis, urinary tract infections (UTIs), meningitis, and other infections in humans.[7][8] Several virulence factors are thought to contribute to E. faecalis infections. A plasmid-encoded hemolysin, called the cytolysin, is important for pathogenesis in animal models of infection, and the cytolysin in combination with high-level gentamicin resistance is associated with a five-fold increase in risk of death in human bacteremia patients.[9][10][11] A plasmid-encoded adhesin[12] called "aggregation substance" is also important for virulence in animal models of infection.[10][13]
E. faecalis contains a tyrosine decarboxylase enzyme capable of decarboxylating L-dopa, a crucial drug in the treatment of Parkinson's disease. If L-dopa is decarboxylated in the gut microbiome, it cannot pass through the blood-brain barrier and be decarboxylated in the brain to become dopamine.[14]
Antibacterial resistance
Multi drug resistance
E. faecalis is usually resistant to many commonly used antimicrobial agents (aminoglycosides, aztreonam and quinolones.[15] The resistance is mediated by the presence of multiple genes related to drug resistance in the chromosome or plasmid.[3]
Resistance to vancomycin in E. faecalis is becoming more common.[16][17] Treatment options for vancomycin-resistant E. faecalis include nitrofurantoin (in the case of uncomplicated UTIs),[18] linezolid, quinupristin, tigecycline[15] and daptomycin, although ampicillin is preferred if the bacteria are susceptible.[19] Quinupristin/dalfopristin can be used to treat Enterococcus faecium but not E. faecalis.[19]
In root-canal treatments, NaOCl and chlorhexidine (CHX) are used to fight E. faecalis before isolating the canal. However, recent studies determined that NaOCl or CHX showed low ability to eliminate E. faecalis.[20]
Development of antibiotic resistance
Combined drug therapies
According to one study combined drug therapy has shown some efficacy in cases of severe infections (e.g. heart valves infections) against susceptible strains of E. faecalis. Ampicillin- and vancomycin-sensitive E. faecalis (lacking high-level resistance to aminoglycosides) strains can be treated by gentamicin and ampicillin antibiotics. A less nephrotoxic combination of ampicillin and ceftriaxone (even though E. faecalis is resistant to cephalosporins, ceftriaxone is working synergistically with ampicillin) may be used alternatively for ampicillin-susceptible E. faecalis.[21]
Daptomycin or linezolid may also show efficacy in case ampicillin and vancomycin resistance.[21]
A combination of penicillin and streptomycin therapy was used in the past.[21]
Tedizolid, telavancin, dalbavancin, and oritavancin antibiotics are FDA approved as treatments against EF.[15]
Survival and virulence factors
- Endures prolonged periods of nutritional deprivation
- Binds to dentin and proficiently spreads into dentinal tubules via chain propagation
- Alters host responses
- Suppresses the action of lymphocytes
- Possesses lytic enzymes, cytolysin, aggregation substance, pheromones, and lipoteichoic acid
- Utilizes serum as a nutritional source
- Produces extracellular superoxide under selected growth conditions that can generate chromosomal instability in mammalian cells[22][23]
- Resists intracanal medicaments (e.g. calcium hydroxide), although a study proposes elimination from root canals after using a mixture of a tetracycline isomer, an acid, and a detergent[24]
- Maintains pH homeostasis
- Properties of dentin lessen the effect of calcium hydroxide
- Competes with other cells
- Forms a biofilm[6]
- Activates the host protease plasminogen in a fashion that increases local tissue destruction[25]
DNA repair
In human blood, E. faecalis is subjected to conditions that damage its DNA, but this damage can be tolerated by the use of DNA repair processes.[26] This damage tolerance depends, in part, on the two protein complex RexAB, encoded by the E. faecalis genome, that is employed in the recombinational repair of DNA double-strand breaks.[26]
Historical
Prior to 1984, enterococci were members of the genus Streptococcus; thus, E. faecalis was known as Streptococcus faecalis.[27]
In 2013, a combination of cold denaturation and NMR spectroscopy was used to show detailed insights into the unfolding of the E. faecalis homodimeric repressor protein CylR2.[28]
Genome structure
The E. faecalis genome consists of 3.22 million base pairs with 3,113 protein-coding genes.[29]
Treatment research
Glutamate racemase, hydroxymethylglutaryl-CoA synthase, diphosphomevalonate decarboxylase, topoisomerase DNA gyrase B, D-alanine—D-serine ligase, alanine racemase, phosphate acetyltransferase, NADH peroxidase,Phosphopantetheine adenylyltransferase (PPAT), acyl carrier protein, 3‐Dehydroquinate dehydratase and Deoxynucleotide triphosphate triphosphohydrolase are all potential molecules that may be used for treating EF infections.[15]
Small RNA
Bacterial small RNAs play important roles in many cellular processes; 11 small RNAs have been experimentally characterised in E. faecalis V583 and detected in various growth phases.[30] Five of them have been shown to be involved in stress response and virulence.[31]
A genome-wide sRNA study suggested that some sRNAs are linked to the antibiotic resistance and stress response in another Enteroccocus: E. faecium.[32]
Swimming pool contamination
Indicators of recreational water quality
Because E. faecalis is a common fecal bacterium in humans, recreational water facilities (such as swimming pools and beaches that allow visitors to swim in the ocean) often measure the concentrations of E. faecalis to assess the quality of their water. The higher the concentration, the worse the quality of the water. The practice of using E. faecalis as a quality indicator is recommended by the World Health Organization (WHO) as well as many developed countries after multiple studies have reported that higher concentrations of E. faecalis correlate to greater percentages of swimmer illness. This correlation exists in both freshwater and marine environments, so measuring E. faecalis concentrations to determine water quality applies to all recreational waters. However, the correlation does not imply that E. faecalis is the ultimate cause of swimmer illnesses. One alternative explanation is that higher levels of E. faecalis correspond to higher levels of human viruses, which cause sickness in swimmers. Although this claim may sound plausible, there is currently little evidence that establishes the link between E. faecalis and human virus (or other pathogens) levels. Thus, despite the strong correlation between E. faecalis and water quality, more research is needed to determine the causal relationship of this correlation.[33]
Human shedding
For recreational waters near or at beaches, E. faecalis can come from multiple sources, such as the sand and human bodies. Determining the sources of E. faecalis is crucial for controlling water contamination, though often the sources are non-point (for example, human bathers). As such, one study looked at how much E. faecalis is shed from bathers at the beach. The first group of participants immersed themselves in a large pool with marine water for 4 cycles of 15 minutes, both with and without contacting sand beforehand. The result shows a decrease in E. faecalis levels for each cycle, suggesting that people shed the most bacteria when they first get into a pool. The second group of participants entered small, individual pools after contact with beach sand, and researchers collected data on how much E. faecalis in the pool came from the sand brought by the participants and how much came from the participants’ shedding. The result shows that E. faecalis from the sand is very small compared to that from human shedding. Although this result may not apply to all sand types, a tentative conclusion is that human shedding is a major non-point source of E. faecalis in recreational waters.[34]
See also
References
- de Almeida CV, Taddei A, Amedei A (2018-01-01). "The controversial role of Enterococcus faecalis in colorectal cancer". Therapeutic Advances in Gastroenterology. SAGE Publications. 11: 1756284818783606. doi:10.1177/1756284818783606. PMC 6044108. PMID 30013618.
- Ryan KJ, Ray CG, eds. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 294–295. ISBN 0-8385-8529-9.
- Panthee S, Paudel A, Hamamoto H, Ogasawara AA, Iwasa T, Blom J, Sekimizu K (May 2021). "Complete genome sequence and comparative genomic analysis of Enterococcus faecalis EF-2001, a probiotic bacterium". Genomics. 113 (3): 1534–1542. doi:10.1016/j.ygeno.2021.03.021. PMID 33771633.
- Molander A, Reit C, Dahlén G, Kvist T (January 1998). "Microbiological status of root-filled teeth with apical periodontitis". International Endodontic Journal. 31 (1): 1–7. doi:10.1046/j.1365-2591.1998.t01-1-00111.x. PMID 9823122.
- Rôças IN, Siqueira JF, Santos KR (May 2004). "Association of Enterococcus faecalis with different forms of periradicular diseases". Journal of Endodontics. 30 (5): 315–320. doi:10.1097/00004770-200405000-00004. PMID 15107642.
- Stuart CH, Schwartz SA, Beeson TJ, Owatz CB (February 2006). "Enterococcus faecalis: its role in root canal treatment failure and current concepts in retreatment". Journal of Endodontics. 32 (2): 93–98. doi:10.1016/j.joen.2005.10.049. PMID 16427453.
- Murray BE (January 1990). "The life and times of the Enterococcus". Clinical Microbiology Reviews. 3 (1): 46–65. doi:10.1128/cmr.3.1.46. PMC 358140. PMID 2404568.
- Hidron AI, Edwards JR, Patel J, Horan TC, Sievert DM, Pollock DA, Fridkin SK (November 2008). "NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006-2007". Infection Control and Hospital Epidemiology. 29 (11): 996–1011. doi:10.1086/591861. PMID 18947320. S2CID 205988392.
- Huycke MM, Spiegel CA, Gilmore MS (August 1991). "Bacteremia caused by hemolytic, high-level gentamicin-resistant Enterococcus faecalis". Antimicrobial Agents and Chemotherapy. 35 (8): 1626–1634. doi:10.1128/aac.35.8.1626. PMC 245231. PMID 1929336.
- Chow JW, Thal LA, Perri MB, Vazquez JA, Donabedian SM, Clewell DB, Zervos MJ (November 1993). "Plasmid-associated hemolysin and aggregation substance production contribute to virulence in experimental enterococcal endocarditis". Antimicrobial Agents and Chemotherapy. 37 (11): 2474–2477. doi:10.1128/aac.37.11.2474. PMC 192412. PMID 8285637.
- Ike Y, Hashimoto H, Clewell DB (August 1984). "Hemolysin of Streptococcus faecalis subspecies zymogenes contributes to virulence in mice". Infection and Immunity. 45 (2): 528–530. doi:10.1128/IAI.45.2.528-530.1984. PMC 263283. PMID 6086531.
- Kreft B, Marre R, Schramm U, Wirth R (January 1992). "Aggregation substance of Enterococcus faecalis mediates adhesion to cultured renal tubular cells". Infection and Immunity. 60 (1): 25–30. doi:10.1128/IAI.60.1.25-30.1992. PMC 257498. PMID 1729187.
- Hirt H, Schlievert PM, Dunny GM (February 2002). "In vivo induction of virulence and antibiotic resistance transfer in Enterococcus faecalis mediated by the sex pheromone-sensing system of pCF10". Infection and Immunity. 70 (2): 716–723. doi:10.1128/iai.70.2.716-723.2002. PMC 127697. PMID 11796604.
- Maini Rekdal V, Bess EN, Bisanz JE, Turnbaugh PJ, Balskus EP (June 2019). "Discovery and inhibition of an interspecies gut bacterial pathway for Levodopa metabolism". Science. 364 (6445): eaau6323. doi:10.1126/science.aau6323. PMC 7745125. PMID 31196984.
- Singh H, Das S, Yadav J, Srivastava VK, Jyoti A, Kaushik S (October 2019). "In search of novel protein drug targets for treatment of Enterococcus faecalis infections". Chemical Biology & Drug Design. Wiley. 94 (4): 1721–1739. doi:10.1111/cbdd.13582. PMID 31260188. S2CID 195756723.
- Amyes SG (May 2007). "Enterococci and streptococci". International Journal of Antimicrobial Agents. 29 (Suppl 3): S43–S52. doi:10.1016/S0924-8579(07)72177-5. PMID 17659211.
- Courvalin P (January 2006). "Vancomycin resistance in gram-positive cocci". Clinical Infectious Diseases. 42 (Suppl 1): S25–S34. doi:10.1086/491711. PMID 16323116.
- Zhanel GG, Hoban DJ, Karlowsky JA (January 2001). "Nitrofurantoin is active against vancomycin-resistant enterococci". Antimicrobial Agents and Chemotherapy. 45 (1): 324–326. doi:10.1128/AAC.45.1.324-326.2001. PMC 90284. PMID 11120989.
- Arias CA, Contreras GA, Murray BE (June 2010). "Management of multidrug-resistant enterococcal infections". Clinical Microbiology and Infection. 16 (6): 555–562. doi:10.1111/j.1469-0691.2010.03214.x. PMC 3686902. PMID 20569266.
- Estrela C, Silva JA, de Alencar AH, Leles CR, Decurcio DA (December 2008). "Efficacy of sodium hypochlorite and chlorhexidine against Enterococcus faecalis--a systematic review". Journal of Applied Oral Science. 16 (6): 364–368. doi:10.1590/s1678-77572008000600002. PMC 4327704. PMID 19082392.
- Dubin K, Pamer EG (2018). "Enterococci and Their Interactions with the Intestinal Microbiome". In Britton RA, Cani PD (eds.). Bugs as Drugs. pp. 309–330. doi:10.1128/microbiolspec.BAD-0014-2016. ISBN 978-1-55581-969-9. PMC 5691600. PMID 29125098.
{{cite book}}:|journal=ignored (help) - Huycke MM, Moore D, Joyce W, Wise P, Shepard L, Kotake Y, Gilmore MS (November 2001). "Extracellular superoxide production by Enterococcus faecalis requires demethylmenaquinone and is attenuated by functional terminal quinol oxidases". Molecular Microbiology. 42 (3): 729–740. doi:10.1046/j.1365-2958.2001.02638.x. PMID 11722738. S2CID 25075356.
- Wang X, Huycke MM (February 2007). "Extracellular superoxide production by Enterococcus faecalis promotes chromosomal instability in mammalian cells". Gastroenterology. 132 (2): 551–561. doi:10.1053/j.gastro.2006.11.040. PMID 17258726.
- Shabahang S, Pouresmail M, Torabinejad M (July 2003). "In vitro antimicrobial efficacy of MTAD and sodium hypochlorite". Journal of Endodontics. 29 (7): 450–452. doi:10.1097/00004770-200307000-00006. PMID 12877261.
- Jacobson RA, Wienholts K, Williamson AJ, Gaines S, Hyoju S, van Goor H, et al. (January 2020). "Enterococcus faecalis exploits the human fibrinolytic system to drive excess collagenolysis: implications in gut healing and identification of druggable targets". American Journal of Physiology. Gastrointestinal and Liver Physiology. 318 (1): G1–G9. doi:10.1152/ajpgi.00236.2019. PMC 6985841. PMID 31604031.
- Ha, K. P.; Clarke, R. S.; Kim, G. L.; Brittan, J. L.; Rowley, J. E.; Mavridou DAI; Parker, D.; Clarke, T. B.; Nobbs, A. H.; Edwards, A. M. (2020). "Staphylococcal DNA Repair is Required for Infection". mBio. 11 (6). doi:10.1128/mBio.02288-20. PMC 7683395. PMID 33203752.
- Schleifer KH, Kilpper-Balz R (1 January 1984). "Transfer of Streptococcus faecalis and Streptococcus faecium to the Genus Enterococcus nom. rev. as Enterococcus faecalis comb. nov. and Enterococcus faecium comb. nov". International Journal of Systematic Bacteriology. 34 (1): 31–34. doi:10.1099/00207713-34-1-31.
- Jaremko M, Jaremko Ł, Kim HY, Cho MK, Schwieters CD, Giller K, et al. (April 2013). "Cold denaturation of a protein dimer monitored at atomic resolution". Nature Chemical Biology. 9 (4): 264–270. doi:10.1038/nchembio.1181. PMC 5521822. PMID 23396077.
- Paulsen IT, Banerjei L, Myers GS, Nelson KE, Seshadri R, Read TD, et al. (March 2003). "Role of mobile DNA in the evolution of vancomycin-resistant Enterococcus faecalis". Science. 299 (5615): 2071–2074. Bibcode:2003Sci...299.2071P. doi:10.1126/science.1080613. PMID 12663927. S2CID 45480495.
- Shioya K, Michaux C, Kuenne C, Hain T, Verneuil N, Budin-Verneuil A, et al. (2 September 2011). "Genome-wide identification of small RNAs in the opportunistic pathogen Enterococcus faecalis V583". PLOS ONE. 6 (9): e23948. Bibcode:2011PLoSO...623948S. doi:10.1371/journal.pone.0023948. PMC 3166299. PMID 21912655.
- Michaux C, Hartke A, Martini C, Reiss S, Albrecht D, Budin-Verneuil A, et al. (September 2014). "Involvement of Enterococcus faecalis small RNAs in stress response and virulence". Infection and Immunity. 82 (9): 3599–3611. doi:10.1128/IAI.01900-14. PMC 4187846. PMID 24914223.
- Sinel C, Augagneur Y, Sassi M, Bronsard J, Cacaci M, Guérin F, et al. (September 2017). "Small RNAs in vancomycin-resistant Enterococcus faecium involved in daptomycin response and resistance". Scientific Reports. 7 (1): 11067. Bibcode:2017NatSR...711067S. doi:10.1038/s41598-017-11265-2. PMC 5593968. PMID 28894187.
- Boehm AB, Sassoubre LM (2014), Gilmore MS, Clewell DB, Ike Y, Shankar N (eds.), "Enterococci as Indicators of Environmental Fecal Contamination", Enterococci: From Commensals to Leading Causes of Drug Resistant Infection, Boston: Massachusetts Eye and Ear Infirmary, PMID 24649503, retrieved 2023-05-08
- Elmir SM, Wright ME, Abdelzaher A, Solo-Gabriele HM, Fleming LE, Miller G, et al. (January 2007). "Quantitative evaluation of bacteria released by bathers in a marine water". Water Research. 41 (1): 3–10. Bibcode:2007WatRe..41....3E. doi:10.1016/j.watres.2006.10.005. PMC 2633726. PMID 17113123.