Selective norepinephrine reuptake inhibitor
Selective norepinephrine reuptake inhibitors (sNRIs) are a class of drugs that have been marketed as antidepressants and are used for various mental disorders, mainly depression and attention-deficit hyperactivity disorder (ADHD). The norepinephrine transporter (NET) serves as the fundamental mechanism for the inactivation of noradrenergic signaling because of the NET termination in the reuptake of norepinephrine (NE). The selectivity and mechanism of action for the NRI drugs remain mostly unresolved and, to date, only a limited number of NRI-selective inhibitors are available. The first commercially available selective NRI was the drug reboxetine (Edronax), developed as a first-line therapy for major depressive disorder. Atomoxetine (Strattera) is another potent and selective NRI which is also effective and well tolerated for the treatment of ADHD in adults; it may also be a new treatment option for adults with ADHD, particularly for those patients at risk of substance abuse.
Medical uses
- Atomoxetine is sold under the brand name Strattera and was first approved for medical use in the United States in 2002.[1] Its indication is for the treatment of attention deficit hyperactivity disorder (ADHD) in kids over 6 years of age, adolescents and adults.[2] Atomoxetine selectively inhibits norepinephrine reuptake by blocking the presynaptic norepinephrine transporter (NET) in the brain. Research has suggested that it also inhibits the reuptake of serotonin by binding to the selective serotonin transporter. However it is not known whether the therapeutic effects of atomoxetine is due to its blockage of the NET or both norepinephrine- and serotonin transporters.[1]
- Reboxetine is the active ingredient, sold under the brand name Edronax.[3] Reboxetine is a selective norepinephrine reuptake inhibitor and acts by binding to the NET and block the reuptake of norepinephrine in the extracellular fluids. Its indication is for acute treatment of depression or major depression disorder. Reboxetine was first approved for marketing in Europe in 1997, however, in the United States its application for approval was rejected.[4]
| Medication | Brand name | Medical uses | Introduced | Chemical structure |
|---|---|---|---|---|
| Atomoxetine | Strattera | Attention deficit hyperactivity disorder (ADHD) | 2002 | 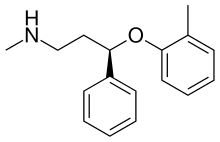 |
| Reboxetine | Edronax | Major depression disorder | 1997 | 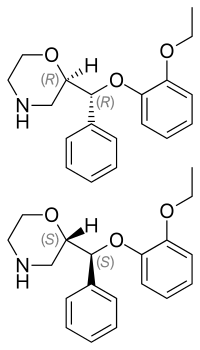 |
Adverse effects
Side effects
Selective NRIs are generally well tolerated but the most common side effects reported are headache, dry mouth, abdominal pain, loss of appetite, nausea, vomiting and drowsiness. An increase in heart rate and blood pressure have been reported but are usually not clinically important. Sexual adverse effects are mostly related to male arousal difficulties and decreased libido in both men and women, but they are significantly less common than with serotonergic drugs. Other side effects are urinary retention, constipation, sweating and insomnia. What can be considered serious side effects are thoughts of suicide, aggressiveness and hallucinations.[5][6][7]
Interactions
If people are using sNRI drugs they should not take MAO inhibitors at the same time. That can increase the plasma concentration of NRIs in the body.
Beware of taking atomoxetine in combination with:[8]
- CYP2D6 inhibitors (e.g., fluoxetine, paroxetine and quinidine) can increase exposure for atomoxetine and it can also increase atomoxetine steady-state plasma concentration.
- Antihypertensive drugs because it can possibly increase the blood pressure
- β2-agonist e.g. albuterol because it may increase the efficacy of albuterol on the cardiovascular system.
- Medicines that affect norepinephrine (e.g. venlafaxine, imipramine, mirtazapine) should be used with caution when administered with atomoxetine due to possible synergy or synergistic effects on pharmacodynamic effects.
Beware of taking reboxetine in combination with:[9]
- Antifungals, e.g. ketoconazole.
- Antibiotics, e.g. erythromycin, rifampicin.
- Ergot derivatives used to treat migraine or Parkinson's disease may cause an increase in blood pressure.
- Any potassium-depleting diuretics (medicines for eliminating water), e.g. thiazides.
- Carbamazepine and phenobarbital, medicines used to control fits or seizures.
- Herbal medicines that contains St. John's Wort.
Contraindications
A few contraindications should be taken into account for atomoxetine. The first one is hypersensitivity but patients known to be hypersensitive to atomoxetine or other constituents of the product should avoid using it. MAO inhibitor (MAOI) should also be taken into account for contraindications. Atomoxetine should not be taken within 2 weeks after discontinuing an MAOI or completely avoid taking MAOI. The same applies to treatment with an MAOI, that it should not be initiated within 2 weeks after discontinuing atomoxetine. Reactions may occur when atomoxetine and drugs that affect brain monoamine concentration are given concurrently or in close proximity, serious and sometimes fatal reactions. Examples of reactions are hyperthermia, inflexibility, myoclonus and altered mental status that include extreme agitation, possibly progressing to delirium and coma. Increased risk of mydriasis was associated with Strattera use in clinical trials. Therefore, the use of Strattera is not recommended in patients with narrow angle glaucoma. Patients with pheochromocytoma or a history of pheochromocytoma should not take Strattera because serious reactions (elevated blood pressure and tachyarrhythmia) have been reported in patients who received Strattera. Last but not least, patients with severe cardiac or vascular disorders should not be using Strattera.[8]
The only contraindication that is reported in the IMB Micromedex database is prior hypersensitivity to the active compound, reboxetine.[10]
Pharmacology
Role of norepinephrine
Norepinephrine (NE), also known as noradrenaline, is a neurotransmitter that is released predominantly from the ends of sympathetic nerve fibers.[11] The sympathetic nervous system is stimulated in fearful situations and elicits the “fight or flight” response both in animals and humans.[12] This stimulus causes the release of catecholamines such as NE. The chemical class of catecholamines has positive chronotropic, inotropic and dromotropic effects which lead to increased heart rate, blood pressure and cardiac output.[13] NE is one of the crucial neurotransmitters in the central nervous system (CNS) and plays an important role in regulating blood pressure, energy metabolism and controlling flexor muscles.[14] The substance has involvement in sleep and mood regulation, expression of behavior and the general degree of alertness and arousal.[11] In the face of a threat, whether it's real or perceived, NE being the most prominent receptor modulator activates behavioral adaptions to maintain homeostasis. The physiological responses in these threatening situation creates emotions of stress and acute anxiety. Responses such as dilatation of bronchioles and pupils, increased heart rate and kidney renin secretion, constricted blood vessels and inhibited peristalsis.[12] Norepinephrine is biosynthesized from the amino acid precursor tyrosine and then is sequentially hydroxylated to dihydroxyphenylalanine, also known as Dopa. Decarboxylation on Dopa generates the neurotransmitter dopamine, afterward when hydroxylated it produces norepinephrine.[11]
Role of norepinephrine transporter (NET)
Approximately 90% of released NE from the sympathetic nerve fibers is taken up again by postganglionic adrenergic neurons through the protein NET. The reuptake of NE is either repackaged into vesicles or degraded by the enzyme monoamine oxidase (MAO).[14][15] The NET is located in the plasma membrane of noradrenergic neurons and serves as the fundamental mechanism by terminating the biological effects of NE in the synapse. The NE inactivation process, when taken up by the NET, is crucial in preventing too much increase in the NE concentration in the synaptic cleft. The reuptake of NE is competitive with various naturally occurring amines and drugs.[11]
Mechanism of action
NET is a target for drugs, that are potent and selective or mixed NET inhibitors (e.g. atomoxetine and reboxetine), named NRI, have been successfully developed to treat various mental disorders, but unfortunately also drugs of abuse (e.g. cocaine). The NRI drugs used medically for mental disorders include attention-deficit hyperactivity disorder (ADHD), depression, anxiety disorders, mood disorders, personality disorders, bipolar disorder, psychosexual disorders and schizophrenia.[11] NRI drugs bind to the NET and inhibit the reuptake of NE. These drugs therefore increase the availability of NE for binding to postsynaptic receptors that regulate adrenergic neurotransmission.[16] Selective NRIs blocks only the monoamine transporter NET, excluding the other two monoamine transporters (DAT and SERT) for dopamine and serotonin. Because if the NRI drug affects those other monoamine transporters they would be called nonselective inhibitors. However, the selectivity and mechanism of action for the NRI drugs remain unknown and, to date, only a very limited number of NRI-selective inhibitors are available. Research has shown that these new ligands vary both in the selectivity and potency at each of these three monoamine transporter sites (NET, DAT and SERT). However, those ligands may be of value in clarifying the pharmacological mechanisms, and in the discovery of new selective NRI drugs with fewer side effects.[11]
Pharmacokinetics
| Name of drug | Bioavailability | Protein binding | tmax (hours) | t1/2 (hours) |
|---|---|---|---|---|
| Atomoxetine | 63-94% | 98% | 1 | 4,5-19 |
| Reboxetine | 94% | 96-97% | 2 | 12–12,5 |
- tmax: Time to achieve a maximum plasma concentration
- t1/2: Biological half-life
Atomoxetine
The pharmacokinetics of atomoxetine are similar in children, teenagers and adults. Pharmacokinetics of atomoxetine has not been studied in children younger than 6 years old. Pharmacokinetic studies have shown that atomoxetine capsules and oral solutions are equivalent. Atomoxetine is very water soluble so it absorbed rapidly and completely after oral administration.[17] Atomoxetine reaches Cmax 1 to 2 hours after administration. The bioavailability of atomoxetine after oral administration is 63-94%, it is dependent on individual differences in the first-pass metabolism.[17] Atomoxetine is widely distributed and is highly (98%) bound to plasma proteins, mainly albumin. The volume of distribution for atomoxetine is 0.85 L/kg, with limited partitioning into red blood cells.[17] Atomoxetine is mainly metabolized by the cytochrome P4502D6 (CYP2D6) enzyme system.[17] The main metabolite formed is 4-hydroxyatomoxetine, which glucuronate rapidly. 4-hydroxyatomoxetine is equivalent to atomoxetine but is much lower in plasma.[8] The mean elimination half-life of atomoxetine after oral administration is 3.6 hours in individuals in extensive metabolism and 21 hours in those with a slow metabolism.[8][18] Atomoxetine is excreted mainly as 4-hydroxyatomoxetin-O-glucoronide with urine.[18]
Reboxetine
If 4 mg of reboxetine is taken orally by a healthy adult, the peak levels can be about 130 ng/mL and are achieved within 2 hours after administration.[19] The administration of reboxetine with food delayed the absorption rate by approximately 2 hours while not affecting the extent of absorption. The absolute bioavailability is approximately 94%. Plasma concentrations of reboxetine fell in one exponential phase (monoexponential) with a half-life of about 12 hours. Steady-state is seen within 5 days.[20][21] Reboxetine is 97% protein bound in young people and 92% in the elderly and is distributed into total body water.[21] Radioactivity excreted in the urine corresponds to 78% of the dose. Even though the drug is mainly unchanged in blood circulation (70% of total radioactivity, as the area under the concentration curve (AUC)), only about 10% of the dose is excreted unchanged in the urine.[19] Reboxetine is almost fully metabolised after oral administration. The drug is mainly metabolised through o-dealkylation and oxidation of the morpholine ring and hydroxylation of the ethoxyphenoxy ring.[19] In vitro studies indicate that the CYP450(3A4) enzyme is primarily responsible for the metabolism of reboxetine.[21] The drug is available as a racemic compound. The RR enantiomer is 10 times less potent than the SS enantiomer. The SS enantiomer (more potent) has a plasma level that is two times lower than the urinary excretion.[20] Elimination of reboxetine is mainly via hepatic metabolism (by cytochrome P450 3A4) with a mean terminal half-life of about 12 hours.[21] No significant difference was observed in the terminal half-lives of the RR and SS diastereomers. About 10% of the dose of reboxetine is cleared renally.[20]
Dosage
For adult patients with attention deficit hyperactivity disorder, the initial dose of atomoxetine should be 40 mg daily. The dose should be increased after a minimum of 3 days to a target dose of 80 mg daily as a single dose in the morning. The 80 mg/day can also be taken in two divided doses in the morning and late afternoon. After 2–4 weeks the dose may be increased to 100 mg/day but doses over 100 mg/ day are not suggested.[22]
In the use of atomoxetine in children (6 years or older up to 70 kg) with attention-deficit hyperactivity disorder, acute treatment should be started with approximately 0.5 mg/kg orally daily. The dose should be increased after a minimum of 3 days up to approximately 1.2 mg/kg daily (target dose) as a single or two divided doses (in the morning and late afternoon). For children older than 6 years old, over 70 kg, acute treatment should be started with 40 mg/day orally and increased up to 80 mg/day after a minimum of 3 days. The dose can be taken as a single dose in the morning or in two divided doses (in the morning and late afternoon). After 2–4 weeks the dose can be increased to 100 mg/ daily.[22]
In the use of reboxetine for depression, clinical studies have shown that most patients are treated with an initial dose of reboxetine 8 mg/day, most often as a divided dose. Depending upon patient tolerance and need, the dose can be increased up to 10 mg/day. Doses over 12 mg/day are not recommended. Doses should be adjusted in renal failure, hepatic insufficiency and in geriatric patients.[10]
Structure and function
Structure activity relationship
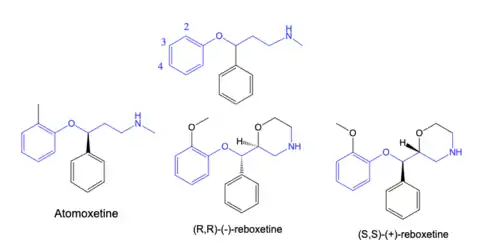
Atomoxetine contains an aryloxy propylamine moiety that has been linked to monoamine reuptake inhibitory activity. It's selectivity to the norepinephrine transporter (NET) is due to its methyl substituent in the 2’ position on the phenyl ring.[23] Research has shown that a methyl group in position 2’ provides more affinity towards NET than a methoxy group in the same position.[24] The amine group of atomoxetine binds to the amino acids of NET with a salt bridge and hydrogen bonds while the phenyl and methylphenyl groups have hydrophobic interactions.[25] Reboxetine has two chiral centers and the active ingredient is a mixture of the (R,R)-(-)- and (S,S)-(+) enantiomers.[26] Reboxetine, like atomoxetine, contains an aryloxy propylamine moiety and has an ethoxy group in position 2’ on the phenyl ring. But the main difference from atomoxetine is the morpholine group instead of a secondary amine.[23] The morpholine group of reboxetine forms a salt bridge and hydrogen bonds with the amino acids of NET. While the phenyl and ethyloxyphenyl groups form hydrophobic interactions.[25]
The aryloxy propylamine moiety is also found in many other monoamine reuptake inhibitors, but the placement of substituents on the phenyl ring determine the selectivity. Compounds with substituents in position 2’ have selectivity for NET. Compounds with substituents in position 4’ are selective serotonin reuptake inhibitors e.g. fluoxetine and paroxetine. Then there is duloxetine which has a phenyl group attached at positions 2’ and 3’ and has a similar affinity for both transporters.[23]
History
In the 1950s, major breakthrough in psychopharmacology occurred around the world. Then throughout the 1960s and 1970s major advances were made in synthesizing and identifying psychoactive drugs which were useful in the treatment of various mental disorders. Here, scientists had realised that these drugs interact with receptors located on neurons that led to changes in neural functioning. The connection was made shortly after the discovery of catecholamines having effects on emotion, relating to depression, and was of wide interest. Discovery was made on the decreased levels of certain neurotransmitters, catecholamines such as norepinephrine, dopamine and serotonin, and their role in the pathogenesis of depression.[27] These past discoveries in psychopharmacology led to the development of antidepressants and a range of drugs with different functions on those neurotransmitters. But a new generation of antidepressants were resulted from the discovery of SSRIs, e.g. fluoxetine. Although SSRIs are a group of effective antidepressant drugs with considerable few severe side effects, they are not universally effective and can also have a few unpleasant side effects, such as weight gain, sleep disturbances and anxiety.[11] Pharmacologically and chemically unrelated to SSRIs, the past four decades, norepinephrine has been asserted to play an important, possibly primary, role in the treatment of mental disorders. This was from the notion that depression was primarily due to norepinephrine deficits, partly based on the fact that drugs that relieve depression increase brain norepinephrine levels.[27] To date, a great number of potent and selective (also mixed) NET inhibitors, e.g. selective NRIs, have been marketed as antidepressants.[11] The first commercially available selective norepinephrine reuptake inhibitor (NRI) was reboxetine (Edronax) and was developed as a first line therapy for major depressive disorder.[28] The selectivity of reboxetine for the NET results in benign side effect profile because the drug is well tolerated.[11] In the laboratories of Chemistry of Farmitalia Carlo Erba (Milan, Italy), reboxetine was synthesized according to the general method described by Melloni et al.[29] In 1993 Kabi Pharmacia, Swedish based pharmaceutical giant, bought Farmitalian and in 2003 Pfizer bought Pharmacia.[30][31] Atomoxetine (Strattera) is another potent and selective NRI which is also effective and well tolerated treatment for adults with ADHD. This drug was the first ADHD treatment to be specially approved for adult use. Studies showed that atomoxetine is a nonstimulant and carries negligible risk of abuse. This discovery was groundbreaking as a beneficial new treatment option for adults with ADHD, specially those patients at risk of substance abuse.[11]
References
- Ding, Y.-S.; Naganawa, M.; Gallezot, J.-D.; Nabulsi, N.; Lin, S.-F.; Ropchan, J.; Weinzimmer, D.; McCarthy, T.J.; Carson, R.E.; Huang, Y.; Laruelle, M. (February 2014). "Clinical doses of atomoxetine significantly occupy both norepinephrine and serotonin transports: Implications on treatment of depression and ADHD". NeuroImage. 86: 164–171. doi:10.1016/j.neuroimage.2013.08.001. PMID 23933039. S2CID 16958660.
- "TGA eBS - Product and Consumer Medicine Information Licence". www.ebs.tga.gov.au.
- Versiani, Marcio; Cassano, Giovanni; Perugi, Giulio; Benedetti, Alessandra; Mastalli, Luigia; Savino, Mario (1 January 2002). "Reboxetine, a Selective Norepinephrine Reuptake Inhibitor, Is an Effective and Well-Tolerated Treatment for Panic Disorder". The Journal of Clinical Psychiatry. 63 (1): 31–37. doi:10.4088/JCP.v63n0107. ISSN 0160-6689. PMID 11838623.
- Eyding, D.; Lelgemann, M.; Grouven, U.; Harter, M.; Kromp, M.; Kaiser, T.; Kerekes, M. F.; Gerken, M.; Wieseler, B. (12 October 2010). "Reboxetine for acute treatment of major depression: systematic review and meta-analysis of published and unpublished placebo and selective serotonin reuptake inhibitor controlled trials". BMJ. 341 (oct12 1): c4737. doi:10.1136/bmj.c4737. PMC 2954275. PMID 20940209.
- Whiskey, Eromona; Taylor, David (19 June 2013). "A review of the adverse effects and safety of noradrenergic antidepressants". Journal of Psychopharmacology. 27 (8): 732–739. doi:10.1177/0269881113492027. PMID 23784737. S2CID 37482892.
- Garnock-Jones, Karly P.; Keating, Gillian M. (2009). "Atomoxetine: A Review of its Use in Attention-Deficit Hyperactivity Disorder in Children and Adolescents". Paediatric Drugs. 11 (3): 203–226. doi:10.2165/00148581-200911030-00005. PMID 19445548. ProQuest 222243344.
- Wells, Barbara G.; Gelenberg, Alan J. (10 September 1981). "Chemistry, Pharmacology, Pharmacokinetics, Adverse Effects, and Efficacy of the Antidepressant Maprotiline Hydrochloride". Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 1 (2): 121–138. doi:10.1002/j.1875-9114.1981.tb03559.x. PMID 6765485. S2CID 19876511.
- "Atomoxetine hydrochloride". Dailymed.
- "Edronax 4 mg tablets" (PDF). The electronic medicines compendium.
- "Reboxetine". www.micromedexsolutions.com.
- Zhou, Jia (December 2004). "Norepinephrine transporter inhibitors and their therapeutic potential". Drugs of the Future. 29 (12): 1235–1244. doi:10.1358/dof.2004.029.12.855246. ISSN 0377-8282. PMC 1518795. PMID 16871320.
- Terbeck, S.; Savulescu, J.; Chesterman, L.P.; Cowen, P.J. (July 2016). "Noradrenaline effects on social behaviour, intergroup relations, and moral decisions". Neuroscience & Biobehavioral Reviews. 66: 54–60. doi:10.1016/j.neubiorev.2016.03.031. PMC 4899514. PMID 27126289.
- Bisogni, Valeria; Pengo, Martino F.; Maiolino, Giuseppe; Rossi, Gian Paolo (2016). "The sympathetic nervous system and catecholamines metabolism in obstructive sleep apnoea". Journal of Thoracic Disease. 8 (2): 243–254. doi:10.3978/j.issn.2072-1439.2015.11.14. ISSN 2072-1439. PMC 4739957. PMID 26904265.
- Boschmann, Michael; Schroeder, Christoph; Christensen, Niels Juel; Tank, Jens; Krupp, Goetz; Biaggioni, Italo; Klaus, Susanne; Sharma, Arya M.; Luft, Friedrich C.; Jordan, Jens (November 2002). "Norepinephrine Transporter Function and Autonomic Control of Metabolism". The Journal of Clinical Endocrinology & Metabolism. 87 (11): 5130–5137. doi:10.1210/jc.2002-020533. PMID 12414883.
- Schroeder, C.; Jordan, J. (1 December 2012). "Norepinephrine transporter function and human cardiovascular disease". American Journal of Physiology. Heart and Circulatory Physiology. 303 (11): H1273–H1282. doi:10.1152/ajpheart.00492.2012. PMID 23023867.
- Mandela, Prashant; Ordway, Gregory A. (2006). "The norepinephrine transporter and its regulation". Journal of Neurochemistry. 97 (2): 310–333. doi:10.1111/j.1471-4159.2006.03717.x. PMID 16539676. S2CID 26772424.
- Sauer, John-Michael; Ring, Barbara J.; Witcher, Jennifer W. (1 June 2005). "Clinical Pharmacokinetics of Atomoxetine". Clinical Pharmacokinetics. 44 (6): 571–590. doi:10.2165/00003088-200544060-00002. ISSN 1179-1926. PMID 15910008. S2CID 25708096.
- "Strattera" (PDF). FDA government.
- "Edronax 4mg Tablets - Summary of Product Characteristics (SmPC) - (emc)". www.medicines.org.uk.
- Dostert, Philippe; Benedetti, Margherita S.; Poggesi, Italo (1 April 1997). "Review of the pharmacokinetics and metabolism of reboxetine, a selective noradrenaline reuptake inhibitor". European Neuropsychopharmacology. 7 (1, Supplement 1): S23–S35. doi:10.1016/S0924-977X(97)00417-3. ISSN 0924-977X. PMID 9169308. S2CID 30214635.
- Fleishaker, Joseph C. (1 December 2000). "Clinical Pharmacokinetics of Reboxetine, a Selective Norepinephrine Reuptake Inhibitor for the Treatment of Patients with Depression". Clinical Pharmacokinetics. 39 (6): 413–427. doi:10.2165/00003088-200039060-00003. ISSN 1179-1926. PMID 11192474. S2CID 7875961.
- "Atomoxetine Hydrochloride". Micromedex.
- Mahaney, Paige E.; Vu, An T.; McComas, Casey C.; Zhang, Puwen; Nogle, Lisa M.; Watts, William L.; Sarkahian, Ani; Leventhal, Liza; Sullivan, Nicole R.; Uveges, Albert J.; Trybulski, Eugene J. (December 2006). "Synthesis and activity of a new class of dual acting norepinephrine and serotonin reuptake inhibitors: 3-(1H-indol-1-yl)-3-arylpropan-1-amines". Bioorganic & Medicinal Chemistry. 14 (24): 8455–8466. doi:10.1016/j.bmc.2006.08.039. PMID 16973367.
- Andersen, Jacob; Kristensen, Anders S.; Bang-Andersen, Benny; Strømgaard, Kristian (2009). "Recent advances in the understanding of the interaction of antidepressant drugs with serotonin and norepinephrine transporters". Chemical Communications (25): 3677–92. doi:10.1039/b903035m. PMID 19557250.
- Zheng, Guoxun; Xue, Weiwei; Wang, Panpan; Yang, Fengyuan; Li, Bo; Li, Xiaofeng; Li, Yinghong; Yao, Xiaojun; Zhu, Feng (27 May 2016). "Exploring the Inhibitory Mechanism of Approved Selective Norepinephrine Reuptake Inhibitors and Reboxetine Enantiomers by Molecular Dynamics Study". Scientific Reports. 6 (1): 26883. Bibcode:2016NatSR...626883Z. doi:10.1038/srep26883. PMC 4882549. PMID 27230580.
- Melloni, P.; Della Torre, A.; Lazzari, E.; Mazzini, G.; Meroni, M. (January 1985). "Configurational studies on 2-[∝-(2-ethoxyphenoxy)benzyl] morpholine fce 20124". Tetrahedron. 41 (7): 1393–1399. doi:10.1016/S0040-4020(01)96541-X.
- Lieberman, Joseph A. (2003). "History of the Use of Antidepressants in Primary Care" (PDF). Primary Care Companion J Clin Psychiatry. 5 (7): 6–10. S2CID 6807291. Archived from the original (PDF) on 2019-10-06.
- Hajós, Mihály; Fleishaker, Joseph C.; Filipiak-Reisner, Jacqueline K.; Brown, Mark T.; Wong, Erik H. F. (7 June 2006). "The Selective Norepinephrine Reuptake Inhibitor Antidepressant Reboxetine: Pharmacological and Clinical Profile". CNS Drug Reviews. 10 (1): 23–44. doi:10.1111/j.1527-3458.2004.tb00002.x. PMC 6741733. PMID 14978512.
- Cocchiara, G.; Battaglia, R.; Pevarello, P.; Benedetti, M. Strolin (July 1991). "Comparison of the disposition and of the metabolic pattern of Reboxetine, a new antidepressant, in the rat, dog, monkey and man". European Journal of Drug Metabolism and Pharmacokinetics. 16 (3): 231–239. doi:10.1007/BF03189965. PMID 1814741. S2CID 874781.
- "Farmitalia bought by Kabi Pharmacia". Annals of Oncology. 4 (5): 345. May 1993. doi:10.1093/oxfordjournals.annonc.a058508.
- "It's official: Pfizer buys Pharmacia - Apr. 16, 2003". money.cnn.com.