Labyrinthine fistula
A labyrinthine fistula is an abnormal opening in the inner ear. This can result in leakage of the perilymph into the middle ear.[1] This includes specifically a perilymph fistula (PLF), an abnormal connection between the fluid of the inner ear and the air-filled middle ear. This is caused by a rupture of the round window or oval window ligaments separating the inner and middle ear.[1]
| Labyrinthine fistula | |
|---|---|
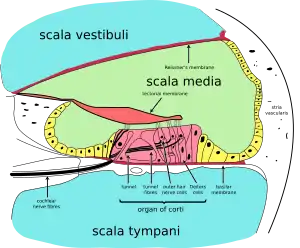 | |
| Cross-section of cochlea. Perilymph is located in the scala tympani and scala vestibuli – the aqua regions at the top and bottom of the diagram. | |
| Specialty | ENT, Neurology |
Another type of labyrinthine fistula is the superior semicircular canal dehiscence, which allows the inner ear to be influenced by the intracranial pressure directly.
Signs and symptoms
PLF usually induces one or all the following pathological states: aural fullness, fluctuating or non-fluctuating hearing loss, tinnitus and dizziness, which may sometimes include vertigo and balance disorders.[2]
Causes
Labyrinthine fistula can be both congenital or develop over time with the thinning of the otic capsule by the persistent pulsations of the intracranial pressures against the bones of the skull. Finally, medical conditions (e.g. cholesteatoma) can result in a labyrinthine fistula.[3] Traumatic events, with excessive pressure changes to the inner ear such as in scuba diving,[4] head trauma, or an extremely loud noise can lead to rupture and leakage.[1] The most common causes of PLF are: head or ear traumas, rapid increases of intracranial pressure, congenital abnormalities (in children), complication of stapedectomy, barotraumas (e.g. slap/suction, scuba diving, skydiving, strong and repetitive nose-blowing or sneezing, heavy lifting).[2]
Diagnosis
When diagnosing, PLF should be differentiated from Ménière's disease. Tympanostomy has been reported to be a way to diagnose[5] and cure PLF.
Treatment
Patients are advised to treat with bed rest and avoiding activities that increase intracranial pressure (i.e. weightlifting, Valsalva maneuver, scuba diving, flying in airplanes) with the hopes of the membrane healing on its own. Appropriate Physical therapy / vestibular rehabilitation techniques can be helpful in managing symptoms of movement sensitivity.[1]
References
- O'Sullivan, Susan B. (2007). Physical Rehabilitation (Fifth ed.). Philadelphia: Davis Company. p. 1024.
- Sarna B, Abouzari M, Merna C, Jamshidi S, Saber T, Djalilian H (2020). "Perilymphatic fistula: a review of classification, etiology, diagnosis and treatment". Frontiers in Neurology. 11. doi:10.3389/fneur.2020.01046. PMID 33041986.
- Chen Z, Wu Y, Shi H, et al. (June 2009). "Surgical treatment of labyrinthine fistula caused by cholesteatoma with semicircular canal occlusion". Acta Otolaryngol. 130 (1): 75–8. doi:10.3109/00016480902875083. PMID 20082558.
- Donoghue, P; Knight, J. "The causation of perilymph fistulae in divers". Journal of the South Pacific Underwater Medicine Society. 10 (2): 13–14. Archived from the original on September 22, 2013. Retrieved 2013-09-22.
{{cite journal}}: CS1 maint: unfit URL (link) - Goto F, Ogawa K, Kunihiro T, Kurashima K, Kobayashi H, Kanzaki J (January 2001). "Perilymph fistula--45 case analysis". Auris Nasus Larynx. 28 (1): 29–33. doi:10.1016/S0385-8146(00)00089-4. PMID 11137360.