Cataract
A cataract is a cloudy area in the lens of the eye that leads to a decrease in vision.[1][7] Cataracts often develop slowly and can affect one or both eyes.[1] Symptoms may include faded colours, blurry or double vision, halos around light, trouble with bright lights, and difficulty seeing at night.[1] This may result in trouble driving, reading, or recognizing faces.[8] Poor vision caused by cataracts may also result in an increased risk of falling and depression.[2] Cataracts cause 51% of all cases of blindness and 33% of visual impairment worldwide.[3][9]
| Cataract | |
|---|---|
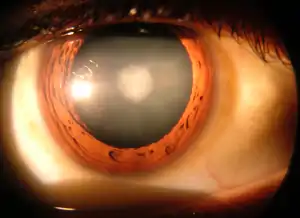 | |
| Magnified view of a cataract seen on examination with a slit lamp | |
| Specialty | Ophthalmology, Optometry |
| Symptoms | Faded colors, blurry vision, halos around light, trouble with bright lights, trouble seeing at night[1] |
| Complications | Falling, depression, blindness[2][3] |
| Usual onset | Gradual[1] |
| Causes | Aging, trauma, radiation exposure, following eye surgery, genetic[1][4][5] |
| Risk factors | Diabetes, smoking tobacco, prolonged exposure to sunlight, alcohol[1] |
| Diagnostic method | Eye examination[1] |
| Prevention | Sunglasses, proper diet, not smoking[1] |
| Treatment | Glasses, cataract surgery[1] |
| Frequency | 60 million (2015)[6] |
Cataracts are most commonly due to aging but may also occur due to trauma or radiation exposure, be present from birth, or occur following eye surgery for other problems.[1][4] Risk factors include diabetes, longstanding use of corticosteroid medication, smoking tobacco, prolonged exposure to sunlight, and alcohol.[1] The underlying mechanism involves accumulation of clumps of protein or yellow-brown pigment in the lens that reduces transmission of light to the retina at the back of the eye.[1] Diagnosis is by an eye examination.[1]
Wearing sunglasses and a wide brimmed hat, eating leafy vegetables and fruits, and avoiding smoking may reduce the risk of developing cataracts, or slow down the process.[1][10] Early on the symptoms may be improved with glasses.[1] If this does not help, surgery to remove the cloudy lens and replace it with an artificial lens is the only effective treatment.[1] Cataract surgery is not readily available in many countries, and surgery is needed only if the cataracts are causing problems and generally results in an improved quality of life.[1][11][4][12]
About 20 million people worldwide are blind due to cataracts.[4] It is the cause of approximately 5% of blindness in the United States and nearly 60% of blindness in parts of Africa and South America.[12] Blindness from cataracts occurs in about 10 to 40 per 100,000 children in the developing world, and 1 to 4 per 100,000 children in the developed world.[7] Cataracts become more common with age.[1] In the United States, cataracts occur in 68% of those over the age of 80 years.[13] Additionally they are more common in women, and less common in Hispanic and Black people.[13]
Signs and symptoms


_PHIL_4284_lores.jpg.webp)
Signs and symptoms vary depending on the type of cataract, though considerable overlap occurs. People with nuclear sclerotic or brunescent cataracts often notice a reduction of vision. Nuclear cataracts typically cause greater impairment of distance vision than of near vision. Those with posterior subcapsular cataracts usually complain of glare as their major symptom.[14]
The severity of cataract formation, assuming no other eye disease is present, is judged primarily by a visual acuity test. Other symptoms include frequent changes of glasses and colored halos due to hydration of lens.
Congenital cataracts can result in amblyopia if not treated in a timely manner.[15]
Causes
Age
Age is the most common cause of cataracts.[1][4] Lens proteins denature and degrade over time, and this process is accelerated by diseases such as diabetes mellitus and hypertension. Environmental factors, including toxins, radiation, and ultraviolet light have cumulative effects which are worsened by the loss of protective and restorative mechanisms due to alterations in gene expression and chemical processes within the eye.[16]
Oxidative stress is an important pathogenic mechanism in cataract formation.[17] Senile cataracts are associated with a decrease in antioxidant capacity in the lens.[17] An increase in oxidative stress in the lens or a decrease in the ability to remove reactive oxygen species can lead to the lens becoming more opaque.[17]
Trauma
Blunt trauma causes swelling, thickening, and whitening of the lens fibers. While the swelling normally resolves with time, the white color may remain. In severe blunt trauma, or in injuries that penetrate the eye, the capsule in which the lens sits can be damaged. This damage allows fluid from other parts of the eye to rapidly enter the lens leading to swelling and then whitening, obstructing light from reaching the retina at the back of the eye. Cataracts may develop in 0.7 to 8.0% of cases following electrical injuries.[18] Blunt trauma can also result in star- (stellate) or petal-shaped cataracts.[19]
Radiation
Cataracts can arise as an effect of exposure to various types of radiation. X-rays, one form of ionizing radiation, may damage the DNA of lens cells.[20] Ultraviolet light, specifically UVB, has also been shown to cause cataracts, and some evidence indicates sunglasses worn at an early age can slow its development in later life.[21] Microwaves, a type of nonionizing radiation, may cause harm by denaturing protective enzymes (e.g., glutathione peroxidase), by oxidizing protein thiol groups (causing protein aggregation), or by damaging lens cells via thermoelastic expansion.[20] The protein coagulation caused by electric and heat injuries whitens the lens.[16] This same process is what makes the clear albumen of an egg become white and opaque during cooking.
Genetics

The genetic component is strong in the development of cataracts,[22] most commonly through mechanisms that protect and maintain the lens. The presence of cataracts in childhood or early life can occasionally be due to a particular syndrome. Examples of chromosome abnormalities associated with cataracts include 1q21.1 deletion syndrome, cri-du-chat syndrome, Down syndrome, Patau's syndrome, trisomy 18 (Edward's syndrome), and Turner's syndrome, and in the case of neurofibromatosis type 2, juvenile cataract on one or both sides may be noted. Examples of single-gene disorder include Alport's syndrome, Conradi's syndrome, cerebrotendineous xanthomatosis, myotonic dystrophy, and oculocerebrorenal syndrome or Lowe syndrome.
Skin diseases
The skin and the lens have the same embryological origin and so can be affected by similar diseases.[23] Those with atopic dermatitis and eczema occasionally develop shield ulcer cataracts. Ichthyosis is an autosomal recessive disorder associated with cuneiform cataracts and nuclear sclerosis. Basal-cell nevus and pemphigus have similar associations.
Smoking and alcohol
Cigarette smoking has been shown to increase the risk of age-related cataract and nuclear cataract.[24][25] Evidence is conflicting over the effect of alcohol. Some surveys have shown a link, but others which followed people over longer terms have not.[26]
Inadequate vitamin C
Low vitamin C intake and serum levels have been associated with greater cataract rates.[27] However, use of supplements of vitamin C has not demonstrated benefit.[28]
Medications
Some medications, such as systemic, topical, or inhaled corticosteroids, may increase the risk of cataract development.[29][30] Corticosteroids most commonly cause posterior subcapsular cataracts.[30] People with schizophrenia often have risk factors for lens opacities (such as diabetes, hypertension, and poor nutrition). Second-generation antipsychotic medications are unlikely to contribute to cataract formation.[31] Miotics[32] and triparanol may increase the risk.[33]
Post-operative
Nearly every person who undergoes a vitrectomy—without ever having had cataract surgery—will experience progression of nuclear sclerosis after the operation.[34] This may be because the native vitreous humor is different from the solutions used to replace the vitreous (vitreous substitutes), such as BSS Plus.[35] This may also be because the native vitreous humour contains ascorbic acid which helps neutralize oxidative damage to the lens and because conventional vitreous substitutes do not contain ascorbic acid.[36][37] Accordingly, for phakic patients requiring a vitrectomy it is becoming increasingly common for ophthalmologists to offer the vitrectomy combined with prophylactic cataract surgery to prevent cataract formation.[38]
Hyperbaric oxygen therapy
Hyperbaric oxygen therapy (HBOT) is the administration of 100% oxygen at pressures greater than one-atmosphere absolute pressure (1 ATA) for a therapeutic purpose. HBOT can have several side effects, including the long-term development of cataracts. This is rare and generally associated with multiple HBOT exposures over a long period. As it does not usually become symptomatic during HBOT, it may often go unrecognised and is probably under-reported. Evidence is emerging that lifetime dosage of oxygen may be a precipitating factor in the development of age-related cataracts. Nuclear cataracts have been hypothesized to be the end stage of the far better known phenomenon of hyperbaric myopic shift.[39]
Other diseases
|
|
 Sunflower cataract of a forty-year-old male with Wilson's disease and decompensated chronic liver disease
|
Diagnosis
Classification
Cataracts may be partial or complete, stationary or progressive, hard or soft. Histologically, the main types of age-related cataracts are nuclear sclerosis, cortical, and posterior subcapsular.[40][41]
Nuclear sclerosis is the most common type of cataract, and involves the central or 'nuclear' part of the lens. This eventually becomes hard, or 'sclerotic', due to condensation on the lens nucleus and the deposition of brown pigment within the lens. In its advanced stages, it is called a brunescent cataract. In early stages, an increase in sclerosis may cause an increase in refractive index of the lens.[42] This causes a myopic shift (lenticular shift) that decreases hyperopia and enables presbyopic patients to see at near without reading glasses. This is only temporary and is called second sight.
Cortical cataracts are due to the lens cortex (outer layer) becoming opaque. They occur when changes in the fluid contained in the periphery of the lens causes fissuring. When these cataracts are viewed through an ophthalmoscope, or other magnification system, the appearance is similar to white spokes of a wheel. Symptoms often include problems with glare and light scatter at night.[42]
Posterior subcapsular cataracts are cloudy at the back of the lens adjacent to the capsule (or bag) in which the lens sits. Because light becomes more focused toward the back of the lens, they can cause disproportionate symptoms for their size.
An immature cataract has some transparent protein, but with a mature cataract, all the lens protein is opaque. In a hypermature or Morgagnian cataract, the lens proteins have become liquid. Congenital cataract, which may be detected in adulthood, has a different classification and includes lamellar, polar, and sutural cataracts.[43][44]
Cataracts can be classified by using the lens opacities classification system LOCS III. In this system, cataracts are classified based on type as nuclear, cortical, or posterior. The cataracts are further classified based on severity on a scale from 1 to 5. The LOCS III system is highly reproducible.[45]
 Posterior polar cataract of an 8-year-old boy in left eye
Posterior polar cataract of an 8-year-old boy in left eye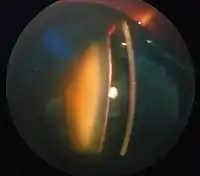 Nuclear sclerosis cataract of a 70-year-old male
Nuclear sclerosis cataract of a 70-year-old male Cortical cataract of a 60-year-old male
Cortical cataract of a 60-year-old male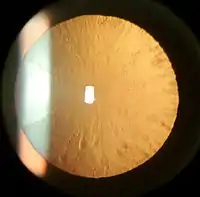 Retroillumination of cortical cataract
Retroillumination of cortical cataract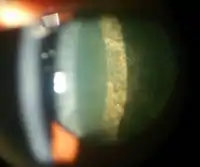 Posterior subcapsular cataract of a 16-year-old girl with type 1 diabetes
Posterior subcapsular cataract of a 16-year-old girl with type 1 diabetes Intumescent cataract of a 55-year-old male
Intumescent cataract of a 55-year-old male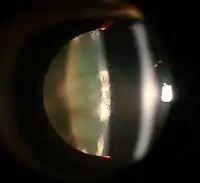 Anterior subcapsular cataract having back shadow
Anterior subcapsular cataract having back shadow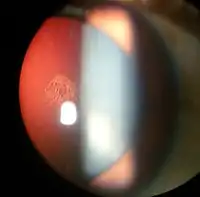 Posterior subcapsular cataract by retroillumination
Posterior subcapsular cataract by retroillumination Nuclear sclerosis and posterior polar cataract of a 60-year-old female
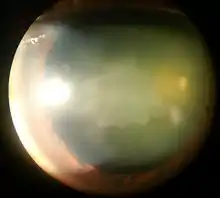
Nuclear sclerosis and posterior polar cataract of a 60-year-old female Dense white mature cataract of a 60-year-old male
Dense white mature cataract of a 60-year-old male Cortical cataract of a melanoderm male
Cortical cataract of a melanoderm male
Prevention
Risk factors such as UVB exposure and smoking can be addressed. Although no means of preventing cataracts has been scientifically proven, wearing sunglasses that block ultraviolet light may slow their development.[46][47] While adequate intake of vitamins A, C, and E may protect against the risk of cataracts, clinical trials have shown no benefit from supplements,[28] although the evidence is mixed, but weakly positive, for a potential protective effect of the carotenoids, lutein and zeaxanthin.[48][49][50]
Treatment
Surgical


The appropriateness of surgery depends on a person's particular functional and visual needs and other risk factors.[51] Cataract removal can be performed at any stage and no longer requires ripening of the lens. Surgery is usually "outpatient" and usually performed using local anesthesia. About 9 of 10 patients can achieve a corrected vision of 20/40 or better after surgery.[42]
Several recent evaluations found that cataract surgery can meet expectations only when significant functional impairment due to cataracts exists before surgery. Visual function estimates such as VF-14 have been found to give more realistic estimates than visual acuity testing alone.[42][52] In some developed countries, a trend to overuse cataract surgery has been noted, which may lead to disappointing results.[53]
Phacoemulsification is the most widely used cataract surgery in the developed world.[54][55] This procedure uses ultrasonic energy to emulsify the cataract lens. Phacoemulsification typically comprises six steps:
- Anaesthetic – The eye is numbed with either a subtenon injection around the eye (see: retrobulbar block) or topical anesthetic eye drops. The former also provides paralysis of the eye muscles.
- Corneal incision – Two cuts are made at the margin of the clear cornea to allow insertion of instruments into the eye.
- Capsulorhexis – A needle or small pair of forceps is used to create a circular hole in the capsule in which the lens sits.
- Phacoemulsification – A handheld ultrasonic probe is used to break up and emulsify the lens into liquid using the energy of ultrasound waves. The resulting 'emulsion' is sucked away.
- Irrigation and aspiration – The cortex, which is the soft outer layer of the cataract, is aspirated or sucked away. Fluid removed is continually replaced with a saline solution to prevent collapse of the structure of the anterior chamber (the front part of the eye).
- Lens insertion – A plastic, foldable lens is inserted into the capsular bag that formerly contained the natural lens. Some surgeons also inject an antibiotic into the eye to reduce the risk of infection. The final step is to inject salt water into the corneal wounds to cause the area to swell and seal the incision.
A Cochrane review found little to no difference in visual acuity as a function of the size of incisions made for phacoemulsification in the range from ≤ 1.5 mm to 3.0 mm.[56] Extracapsular cataract extraction (ECCE) consists of removing the lens manually, but leaving the majority of the capsule intact.[57] The lens is expressed through a 10- to 12-mm incision which is closed with sutures at the end of surgery. ECCE is less frequently performed than phacoemulsification, but can be useful when dealing with very hard cataracts or other situations where emulsification is problematic. Manual small incision cataract surgery (MSICS) has evolved from ECCE. In MSICS, the lens is removed through a self-sealing scleral tunnel wound in the sclera which, ideally, is watertight and does not require suturing. Although "small", the incision is still markedly larger than the portal in phacoemulsification. This surgery is increasingly popular in the developing world where access to phacoemulsification is still limited.
Intracapsular cataract extraction (ICCE) is rarely performed.[58] The lens and surrounding capsule are removed in one piece through a large incision while pressure is applied to the vitreous membrane. The surgery has a high rate of complications.
Prognosis
Postoperative care

.jpg.webp)
The postoperative recovery period (after removing the cataract) is usually short. The patient is usually ambulatory on the day of surgery, but is advised to move cautiously and avoid straining or heavy lifting for about a month. The eye is usually patched on the day of surgery and use of an eye shield at night is often suggested for several days after surgery.[51]
In all types of surgery, the cataractous lens is removed and replaced with an artificial lens, known as an intraocular lens, which stays in the eye permanently. Intraocular lenses are usually monofocal, correcting for either distance or near vision. Multifocal lenses may be implanted to improve near and distance vision simultaneously, but these lenses may increase the chance of unsatisfactory vision.[16]
Complications
Serious complications of cataract surgery include retinal detachment and endophthalmitis.[59] In both cases, patients notice a sudden decrease in vision. In endophthalmitis, patients often describe pain. Retinal detachment frequently presents with unilateral visual field defects, blurring of vision, flashes of light, or floating spots.
The risk of retinal detachment was estimated as about 0.4% within 5.5 years, corresponding to a 2.3-fold risk increase compared to naturally expected incidence, with older studies reporting a substantially higher risk. The incidence is increasing over time in a somewhat linear manner, and the risk increase lasts for at least 20 years after the procedure. Particular risk factors are younger age, male sex, longer axial length, and complications during surgery. In the highest risk group of patients, the incidence of pseudophakic retinal detachment may be as high as 20%.[60][61]
The risk of endophthalmitis occurring after surgery is less than one in 1000.[62]
Corneal edema and cystoid macular edema are less serious but more common, and occur because of persistent swelling at the front of the eye in corneal edema or back of the eye in cystoid macular edema.[63] They are normally the result of excessive inflammation following surgery, and in both cases, patients may notice blurred, foggy vision. They normally improve with time and with application of anti-inflammatory drops. The risk of either occurring is around one in 100. It is unclear whether NSAIDs or corticosteroids are superior at reducing postoperative inflammation.[64]
Posterior capsular opacification, also known as after-cataract, is a condition in which months or years after successful cataract surgery, vision deteriorates or problems with glare and light scattering recur, usually due to thickening of the back or posterior capsule surrounding the implanted lens, so-called 'posterior lens capsule opacification'. Growth of natural lens cells remaining after the natural lens was removed may be the cause, and the younger the patient, the greater the chance of this occurring. Management involves cutting a small, circular area in the posterior capsule with targeted beams of energy from a laser, called Nd:YAG laser capsulotomy, after the type of laser used. The laser can be aimed very accurately, and the small part of the capsule which is cut falls harmlessly to the bottom of the inside of the eye. This procedure leaves sufficient capsule to hold the lens in place, but removes enough to allow light to pass directly through to the retina. Serious side effects are rare.[65] Posterior capsular opacification is common and occurs following up to one in four operations, but these rates are decreasing following the introduction of modern intraocular lenses together with a better understanding of the causes.
Vitreous touch syndrome is a possible complication of intracapsular cataract extraction.[66]
Epidemiology

|
no data
<90
90–180
180–270
270–360
360–450
450–540 |
540–630
630–720
720–810
810–900
900–990
>990
|
Age-related cataracts are responsible for 51% of world blindness, about 20 million people.[68] Globally, cataracts cause moderate to severe disability in 53.8 million (2004), 52.2 million of whom are in low and middle income countries.[69]
In many countries, surgical services are inadequate, and cataracts remain the leading cause of blindness.[68] Even where surgical services are available, low vision associated with cataracts may still be prevalent as a result of long waits for, and barriers to, surgery, such as cost, lack of information and transportation problems.
In the United States, age-related lens changes have been reported in 42% between the ages of 52 and 64,[70] 60% between the ages 65 and 74,[71] and 91% between the ages of 75 and 85.[70] Cataracts affect nearly 22 million Americans age 40 and older. By age 80, more than half of all Americans have cataracts. Direct medical costs for cataract treatment are estimated at $6.8 billion annually.[72]
In the eastern Mediterranean region, cataracts are responsible for over 51% of blindness. Access to eye care in many countries in this region is limited.[73] Childhood-related cataracts are responsible for 5–20% of world childhood blindness.[74]
History
Cataract surgery was first described by the Ayurvedic physician, Suśruta (about 5th century BCE) in Sushruta Samhita in ancient India. Most of the methods mentioned focus on hygiene. Follow-up treatments include bandaging of the eye and covering the eye with warm butter.[75] References to cataracts and their treatment in Ancient Rome are also found in 29 AD in De Medicinae, the work of the Latin encyclopedist Aulus Cornelius Celsus.[76] Archaeological evidence of eye surgery in the Roman era also exists.[77]
Galen of Pergamon (ca. 2nd century CE), a prominent Greek physician, surgeon and philosopher, performed an operation similar to modern cataract surgery. Using a needle-shaped instrument, Galen attempted to remove the cataract-affected lens of the eye.[78]
Muslim ophthalmologist Ammar Al-Mawsili, in his The Book of Choice in Ophthalmology, written circa 1000 CE, wrote of his invention of a syringe and the technique of cataract extraction while experimenting with it on a patient.[79]
In 1468 Abiathar Crescas, a Jewish physician and astrologer of the Crown of Aragon, famously removed the cataracts of King John II of Aragon, restoring his eyesight.
Etymology
"Cataract" is derived from the Latin cataracta, meaning "waterfall", and from the Ancient Greek καταρράκτης (katarrhaktēs), "down-rushing",[80] from καταράσσω (katarassō) meaning "to dash down"[81] (from kata-, "down"; arassein, "to strike, dash").[82][83] As rapidly running water turns white, so the term may have been used metaphorically to describe the similar appearance of mature ocular opacities. In Latin, cataracta had the alternative meaning "portcullis"[84] and the name possibly passed through French to form the English meaning "eye disease" (early 15th century), on the notion of "obstruction".[85] Early Persian physicians called the term nazul-i-ah, or "descent of the water"—vulgarised into waterfall disease or cataract—believing such blindness to be caused by an outpouring of corrupt humour into the eye.[86]
Research
N-Acetylcarnosine drops have been investigated as a medical treatment for cataracts. The drops are believed to work by reducing oxidation and glycation damage in the lens, particularly reducing crystallin crosslinking.[87][88] Some benefit has been shown in small manufacturer-sponsored randomized controlled trials but further independent corroboration is still required.[89]
Femtosecond laser mode-locking, used during cataract surgery, was originally used to cut accurate and predictable flaps in LASIK surgery, and has been introduced to cataract surgery. The incision at the junction of the sclera and cornea and the hole in capsule during capsulorhexis, traditionally made with a handheld blade, needle, and forceps, are dependent on skill and experience of the surgeon. Sophisticated three-dimensional images of the eyes can be used to guide lasers to make these incisions. A Nd:YAG laser can also then break up the cataract as in phacoemulsification.[90]
Stem cells have been used in a clinical trial, with results submitted in 2014 and published in March 2016, for lens regeneration in twelve children under the age of two with cataracts present at birth.[91] The children were followed for six months, so it is unknown what the long-term results have been, and it is unknown if this procedure would work in adults.[91]
See also
- Galactosemic cataract – medical condition
- Intraocular lens – Lens implanted in the eye to treat cataracts or myopia
References
- "Facts About Cataract". September 2009. Archived from the original on 24 May 2015. Retrieved 24 May 2015.
- Gimbel HV, Dardzhikova AA (January 2011). "Consequences of waiting for cataract surgery". Current Opinion in Ophthalmology. 22 (1): 28–30. doi:10.1097/icu.0b013e328341425d. PMID 21076306. S2CID 205670956.
- "Visual impairment and blindness Fact Sheet N°282". August 2014. Archived from the original on 12 May 2015. Retrieved 23 May 2015.
- "Priority eye diseases". Archived from the original on 24 May 2015. Retrieved 24 May 2015.
- Chan WH, Biswas S, Ashworth JL, Lloyd IC (April 2012). "Congenital and infantile cataract: aetiology and management". European Journal of Pediatrics. 171 (4): 625–630. doi:10.1007/s00431-012-1700-1. PMID 22383071. S2CID 195680440.
- Vos, Theo; et al. (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- Pandey SK (2005). Pediatric cataract surgery techniques, complications, and management. Philadelphia: Lippincott Williams & Wilkins. p. 20. ISBN 978-0781743075. Archived from the original on 2015-05-24.
- Allen D, Vasavada A (July 2006). "Cataract and surgery for cataract". BMJ. 333 (7559): 128–132. doi:10.1136/bmj.333.7559.128. PMC 1502210. PMID 16840470.
- Global Data on Visual Impairments 2010 (PDF). WHO. 2012. p. 6. Archived (PDF) from the original on 2015-03-31.
- "Recognizing Cataracts". NIH News in Health. 2017-05-30. Retrieved 2020-02-02.
Try wearing sunglasses or a hat with a brim. Researchers also believe that good nutrition can help reduce the risk of age-related cataract. They recommend eating plenty of green leafy vegetables, fruits, nuts and other healthy foods.
- Lamoureux EL, Fenwick E, Pesudovs K, Tan D (January 2011). "The impact of cataract surgery on quality of life". Current Opinion in Ophthalmology. 22 (1): 19–27. doi:10.1097/icu.0b013e3283414284. PMID 21088580. S2CID 22760161.
- Rao GN, Khanna R, Payal A (January 2011). "The global burden of cataract". Current Opinion in Ophthalmology. 22 (1): 4–9. doi:10.1097/icu.0b013e3283414fc8. PMID 21107260. S2CID 205670997.
- "Cataract Data and Statistics | National Eye Institute". www.nei.nih.gov. Retrieved 2019-11-18.
- "Posterior Supcapsular Cataract". Digital Reference of Ophthalmology. Edward S. Harkness Eye Institute, Department of Ophthalmology of Columbia University. 2003. Archived from the original on 27 March 2013. Retrieved 2 April 2013.
- Mohammadpour M, Shaabani A, Sahraian A, Momenaei B, Tayebi F, Bayat R, Mirshahi R (June 2019). "Updates on managements of pediatric cataract". Journal of Current Ophthalmology. 31 (2): 118–126. doi:10.1016/j.joco.2018.11.005. PMC 6611931. PMID 31317088.
- Duker JS, Yanoff M (2009). Ophthalmology. St. Louis, Mo: Mosby/Elsevier. ISBN 978-0-323-04332-8.
- Hsueh YJ, Chen YN, Tsao YT, Cheng CM, Wu WC, Chen HC. The Pathomechanism, Antioxidant Biomarkers, and Treatment of Oxidative Stress-Related Eye Diseases. Int J Mol Sci. 2022 Jan 23;23(3):1255. doi: 10.3390/ijms23031255. PMID 35163178; PMCID: PMC8835903
- Reddy SC (1999). "Electric cataract: a case report and review of the literature". European Journal of Ophthalmology. 9 (2): 134–138. doi:10.1177/112067219900900211. PMID 10435427. S2CID 45814684.
- Ram J, Gupta R (May 2016). "IMAGES IN CLINICAL MEDICINE. Petaloid Cataract". The New England Journal of Medicine. 374 (18): e22. doi:10.1056/NEJMicm1507349. PMID 27144871.
- Lipman RM, Tripathi BJ, Tripathi RC (1988). "Cataracts induced by microwave and ionizing radiation". Survey of Ophthalmology. 33 (3): 200–210. doi:10.1016/0039-6257(88)90088-4. PMID 3068822.
- Sliney DH (1994). "UV radiation ocular exposure dosimetry". Documenta Ophthalmologica. Advances in Ophthalmology. 88 (3–4): 243–254. doi:10.1007/bf01203678. PMID 7634993. S2CID 8242055.
- Hejtmancik JF, Smaoui N (2003), "Molecular Genetics of Cataract", Genetics in Ophthalmology, Karger Medical and Scientific Publishers, p. 77, ISBN 978-3805575782
- Yanoff M, Duker JS (2009), Ophthalmology, Elsevier Health Sciences, p. 507, ISBN 978-0323043328
- Ye J, He J, Wang C, Wu H, Shi X, Zhang H, Xie J, Lee SY. (2012). "Smoking and risk of age-related cataract: a meta-analysis". Invest Ophthalmol Vis Sci. 53 (7): 3885–95. doi:10.1167/iovs.12-9820. PMID 22599585.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - Beltrán-Zambrano E, García-Lozada D, Ibáñez-Pinilla E. (2019). "Risk of cataract in smokers: A meta-analysis of observational studies". Arch Soc Esp Oftalmol (Engl Ed). 94 (2): 60–74. doi:10.1016/j.oftal.2018.10.020. PMID 30528895. S2CID 155984835.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - Wang S, Wang JJ, Wong TY (2008). "Alcohol and eye diseases". Survey of Ophthalmology. 53 (5): 512–525. doi:10.1016/j.survophthal.2008.06.003. PMID 18929762.
- Wei L, Liang G, Cai C, Lv J (May 2016). "Association of vitamin C with the risk of age-related cataract: a meta-analysis". Acta Ophthalmologica. 94 (3): e170–e176. doi:10.1111/aos.12688. PMID 25735187. S2CID 42785248.
- Mathew MC, Ervin AM, Tao J, Davis RM (June 2012). "Antioxidant vitamin supplementation for preventing and slowing the progression of age-related cataract". The Cochrane Database of Systematic Reviews. 6 (6): CD004567. doi:10.1002/14651858.CD004567.pub2. PMC 4410744. PMID 22696344.
- Weatherall M, Clay J, James K, Perrin K, Shirtcliffe P, Beasley R (September 2009). "Dose-response relationship of inhaled corticosteroids and cataracts: a systematic review and meta-analysis". Respirology. 14 (7): 983–990. doi:10.1111/j.1440-1843.2009.01589.x. PMID 19740259. S2CID 43843511.
- Hodge WG, Whitcher JP, Satariano W (1995). "Risk factors for age-related cataracts". Epidemiologic Reviews. 17 (2): 336–346. doi:10.1093/oxfordjournals.epirev.a036197. PMID 8654515.
- Uçok A, Gaebel W (February 2008). "Side effects of atypical antipsychotics: a brief overview". World Psychiatry. 7 (1): 58–62. doi:10.1002/j.2051-5545.2008.tb00154.x. PMC 2327229. PMID 18458771.
- van den Brûle J, Degueldre F, Galand A (December 1998). "[Drug-induced cataracts]" [Drug-induced cataracts]. Revue Médicale de Liège (in French). 53 (12): 766–769. PMID 9927876.
- "Triperanol". MeSH. National Library of Medicine. Archived from the original on 2015-12-22. Retrieved 2013-02-06.
- Almony A, Holekamp NM, Bai F, Shui YB, Beebe D (March 2012). "Small-gauge vitrectomy does not protect against nuclear sclerotic cataract". Retina. 32 (3): 499–505. doi:10.1097/IAE.0b013e31822529cf. PMID 22392091. S2CID 31308270.
- Kokavec J, Min SH, Tan MH, Gilhotra JS, Newland HS, Durkin SR, et al. (September 2016). "Biochemical analysis of the living human vitreous". Clinical & Experimental Ophthalmology. 44 (7): 597–609. doi:10.1111/ceo.12732. PMID 26891415.
- Donati S, Caprani SM, Airaghi G, Vinciguerra R, Bartalena L, Testa F, et al. (2014). "Vitreous substitutes: the present and the future". BioMed Research International. 2014: 351804. doi:10.1155/2014/351804. PMC 4024399. PMID 24877085.
- Shui YB, Holekamp NM, Kramer BC, Crowley JR, Wilkins MA, Chu F, et al. (April 2009). "The gel state of the vitreous and ascorbate-dependent oxygen consumption: relationship to the etiology of nuclear cataracts". Archives of Ophthalmology. 127 (4): 475–482. doi:10.1001/archophthalmol.2008.621. PMC 2683478. PMID 19365028.
- Jalil A, Steeples L, Subramani S, Bindra MS, Dhawahir-Scala F, Patton N (April 2014). "Microincision cataract surgery combined with vitrectomy: a case series". Eye. 28 (4): 386–389. doi:10.1038/eye.2013.300. PMC 3983625. PMID 24406418.
- Bennett, Michael H.; Cooper, Jeffrey S. (10 August 2022). "Hyperbaric Cataracts". www.ncbi.nlm.nih.gov. StatPearls Publishing LLC. PMID 29261974. Retrieved 27 February 2023.
- "Age Related or Senile Cataract: Pathology, Mechanism and Management". austinpublishinggroup.com. Retrieved 2023-04-24.
- Aliancy, Joah F.; Mamalis, Nick (1995), Kolb, Helga; Fernandez, Eduardo; Nelson, Ralph (eds.), "Crystalline Lens and Cataract", Webvision: The Organization of the Retina and Visual System, Salt Lake City (UT): University of Utah Health Sciences Center, PMID 29356473, retrieved 2023-04-24
- Bollinger KE, Langston RH (March 2008). "What can patients expect from cataract surgery?". Cleveland Clinic Journal of Medicine. 75 (3): 193–96, 199–200. doi:10.3949/ccjm.75.3.193. PMID 18383928. S2CID 27022598.
- Spencer RW, Andelman SY (July 1965). "Steroid cataracts. Posterior subcapsular cataract formation in rheumatoid arthritis patients on long term steroid therapy". Archives of Ophthalmology. 74: 38–41. doi:10.1001/archopht.1965.00970040040009. PMID 14303339.
- Greiner JV, Chylack LT (January 1979). "Posterior subcapsular cataracts: histopathologic study of steroid-associated cataracts". Archives of Ophthalmology. 97 (1): 135–144. doi:10.1001/archopht.1979.01020010069017. PMID 758890.
- Yanoff M, Duker JS (2008). Ophthalmology (3rd ed.). Edinburgh: Mosby. p. 412. ISBN 978-0323057516.
- Neale RE, Purdie JL, Hirst LW, Green AC (November 2003). "Sun exposure as a risk factor for nuclear cataract". Epidemiology. 14 (6): 707–712. doi:10.1097/01.ede.0000086881.84657.98. PMID 14569187. S2CID 40041207.
- Javitt JC, Wang F, West SK (1996). "Blindness due to cataract: epidemiology and prevention". Annual Review of Public Health. 17: 159–177. doi:10.1146/annurev.pu.17.050196.001111. PMID 8724222. Cited in Five-Year Agenda for the National Eye Health Education Program (NEHEP), p. B-2; National Eye Institute, U.S. National Institutes of Health
- Barker FM (August 2010). "Dietary supplementation: effects on visual performance and occurrence of AMD and cataracts". Current Medical Research and Opinion. 26 (8): 2011–2023. doi:10.1185/03007995.2010.494549. PMID 20590393. S2CID 206965363.
- Ma L, Hao ZX, Liu RR, Yu RB, Shi Q, Pan JP (January 2014). "A dose-response meta-analysis of dietary lutein and zeaxanthin intake in relation to risk of age-related cataract". Graefe's Archive for Clinical and Experimental Ophthalmology = Albrecht von Graefes Archiv für Klinische und Experimentelle Ophthalmologie. 252 (1): 63–70. doi:10.1007/s00417-013-2492-3. PMID 24150707. S2CID 13634941.
- Hayashi R (2014-11-01). "The Effects of Lutein in Preventing Cataract Progression". In Babizhayev MA, Li DW, Kasus-Jacobi A, Žorić L, Alió JL (eds.). Studies on the Cornea and Lens. Oxidative Stress in Applied Basic Research and Clinical Practice. pp. 317–26. doi:10.1007/978-1-4939-1935-2_17. ISBN 9781493919345.
- Cunningham ET, Riordan-Eva P (2011). Vaughan & Asbury's general ophthalmology (18th ed.). McGraw-Hill Medical. ISBN 978-0071634205.
- Davis JC, McNeill H, Wasdell M, Chunick S, Bryan S (September 2012). "Focussing both eyes on health outcomes: revisiting cataract surgery". BMC Geriatrics. 12: 50. doi:10.1186/1471-2318-12-50. PMC 3497611. PMID 22943071.

- Black N, Browne J, van der Meulen J, Jamieson L, Copley L, Lewsey J (January 2009). "Is there overutilisation of cataract surgery in England?" (PDF). The British Journal of Ophthalmology. 93 (1): 13–17. doi:10.1136/bjo.2007.136150. PMID 19098042. S2CID 37414146.
- Kim E, Yoon SY, Shin YJ (2014), Studies on the Cornea and Lens, Springer, p. 4, ISBN 978-1493919352
- Pascal H (2013), Essential Principles of Phacoemulsification, JP Medical Ltd, ISBN 978-9962678618
- Jin C, Chen X, Law A, Kang Y, Wang X, Xu W, Yao K (September 2017). "Different-sized incisions for phacoemulsification in age-related cataract". The Cochrane Database of Systematic Reviews. 2017 (9): CD010510. doi:10.1002/14651858.CD010510.pub2. PMC 5665700. PMID 28931202.
- Henderson B (2007), "Extracapsular Cataract Extraction", Essentials of Cataract Surgery, Slack, p. 187, ISBN 978-1556428029
- Goes F (2013), The Eye in History, JP Medical, p. 367, ISBN 978-9350902745
- Naumann GO, Holbach LM, Kruse FE, eds. (2008), "Complications After Cataract Surgery", Applied Pathology for Ophthalmic Microsurgeons, Springer Science & Business, p. 247, ISBN 978-3540683667
- Olsen T, Jeppesen P (2012). "The incidence of retinal detachment after cataract surgery". The Open Ophthalmology Journal. 6: 79–82. doi:10.2174/1874364101206010079. PMC 3447164. PMID 23002414.
- Herrmann W, Helbig H, Heimann H (March 2011). "[Pseudophakic retinal detachment]". Klinische Monatsblätter für Augenheilkunde. 228 (3): 195–200. doi:10.1055/s-0029-1246116. PMID 21374539. S2CID 260192934.
- Behndig A, Montan P, Stenevi U, Kugelberg M, Lundström M (August 2011). "One million cataract surgeries: Swedish National Cataract Register 1992-2009". Journal of Cataract and Refractive Surgery. 37 (8): 1539–1545. doi:10.1016/j.jcrs.2011.05.021. PMID 21782099.
- Gault J, Vander J (2015), Ophthalmology Secrets in Color, Elsevier Health Sciences, p. 221, ISBN 978-0323378024
- Juthani VV, Clearfield E, Chuck RS (July 2017). "Non-steroidal anti-inflammatory drugs versus corticosteroids for controlling inflammation after uncomplicated cataract surgery". The Cochrane Database of Systematic Reviews. 2017 (7): CD010516. doi:10.1002/14651858.CD010516.pub2. PMC 5580934. PMID 28670710.
- "Posterior capsule opacification – why laser treatment is sometimes needed following cataract surgery". rnib.org.uk. 2014-02-19. Archived from the original on 2009-09-17.
- Banerjee K (2006). "A review and clinical evaluation of per-operative and post-operative complications in case of manual small incision cataract surgery and extracapsular cataract extraction with posterior chamber intra-ocular lens implantation" (PDF). Archived from the original (PDF) on 5 June 2014. Retrieved 1 June 2014.
- "Death and DALY estimates for 2004 by cause for WHO Member States" (xls). World Health Organization. who.int. 2004.
- "Priority eye diseases: Cataract". Prevention of Blindness and Visual Impairment. World Health Organization. Archived from the original on 2015-05-24.
- The global burden of disease : 2004 update. Geneva, Switzerland: World Health Organization. 2008. p. 35. ISBN 978-9241563710.
- Sperduto RD, Seigel D (July 1980). "Senile lens and senile macular changes in a population-based sample". American Journal of Ophthalmology. 90 (1): 86–91. doi:10.1016/s0002-9394(14)75081-0. PMID 7395962.
- Kahn HA, Leibowitz HM, Ganley JP, Kini MM, Colton T, Nickerson RS, Dawber TR (July 1977). "The Framingham Eye Study. I. Outline and major prevalence findings". American Journal of Epidemiology. 106 (1): 17–32. doi:10.1093/oxfordjournals.aje.a112428. PMID 879158.
- "Eye Health Statistics at a Glance" (PDF). Archived from the original (PDF) on March 17, 2015.
- "Health Topics: Cataract". World Health Organization – Eastern Mediterranean Regional Office. Archived from the original on 2013-09-27.
- Liu YC, Wilkins M, Kim T, Malyugin B, Mehta JS (August 2017). "Cataracts". Lancet. 390 (10094): 600–612. doi:10.1016/S0140-6736(17)30544-5. PMID 28242111. S2CID 208790600.
- Goes FJ (2013). The Eye in History. JP Medical Ltd. p. 371. ISBN 978-9350902745.
- Celsus AC, Collier GF (1831). De Medicinae. OL 5225311W.
- Elliott J (February 9, 2008). "The Romans carried out cataract ops". BBC News. Archived from the original on February 18, 2008.
- Keele KD (1963). "Galen: On Anatomical Procedures: the Later Books". Med Hist. 7 (1): 85–87. doi:10.1017/s002572730002799x. PMC 1034789.
- Stanley F (1994). Origins of Neuroscience: A History of Explorations Into Brain Function. Oxford University Press. p. 70. ISBN 978-0-19-514694-3.
- Liddell, Henry George; Scott, Robert. "καταρράκτης". A Greek-English Lexicon. Archived from the original on 2012-04-05 – via Perseus.
- Liddell, Henry George; Scott, Robert. "καταράσσω". A Greek-English Lexicon. Archived from the original on 2012-04-04 – via Perseus.
- "cataract". Dictionary.com. Dictionary.com, LLC. Retrieved 1 April 2020.
- "cataract". Oxford Dictionaries. Oxford University Press. Archived from the original on 8 October 2012. Retrieved 1 April 2020.
- Lewis, Charlton T.; Short, Charles. "cataracta". A Latin Dictionary. Archived from the original on 2012-04-04 – via Perseus.
- "cataract". Online Etymology Dictionary. Archived from the original on 2007-10-14.
- Mistaken Science – Topic Powered by eve community Archived 2008-06-22 at the Wayback Machine, Wordcraft Forums, wordcraft.infopop.cc
- Williams DL, Munday P (2006). "The effect of a topical antioxidant formulation including N-acetyl carnosine on canine cataract: a preliminary study". Veterinary Ophthalmology. 9 (5): 311–316. doi:10.1111/j.1463-5224.2006.00492.x. PMID 16939459.
- Guo Y, Yan H (June 2006). "[Preventive effect of carnosine on cataract development]". Yan Ke Xue Bao = Eye Science. 22 (2): 85–88. PMID 17162883.
- Toh T, Morton J, Coxon J, Elder MJ (2007). "Medical treatment of cataract". Clinical & Experimental Ophthalmology. 35 (7): 664–671. doi:10.1111/j.1442-9071.2007.01559.x. PMID 17894689. S2CID 43125880.
- Friedman NJ, Palanker DV, Schuele G, Andersen D, Marcellino G, Seibel BS, et al. (July 2011). "Femtosecond laser capsulotomy". Journal of Cataract and Refractive Surgery. 37 (7): 1189–1198. doi:10.1016/j.jcrs.2011.04.022. PMID 21700099. S2CID 3860204. as PDF Archived 2012-09-14 at the Wayback Machine The authors declare a financial interest in a company producing femtosecond laser equipment.
- "Stem cells used to repair children's eyes after cataracts". NHS. March 10, 2016. Archived from the original on 11 March 2016. Retrieved 11 March 2016.
Further reading
- Truscott RJ, Friedrich MG (December 2019). "Molecular Processes Implicated in Human Age-Related Nuclear Cataract". Investigative Ophthalmology & Visual Science. 60 (15): 5007–5021. doi:10.1167/iovs.19-27535. OCLC 1141250841. PMC 7043214. PMID 31791064.