Achondroplasia
Achondroplasia is a genetic disorder with an autosomal dominant pattern of inheritance whose primary feature is dwarfism.[3] In those with the condition, the arms and legs are short, while the torso is typically of normal length.[3] Those affected have an average adult height of 131 centimetres (4 ft 4 in) for males and 123 centimetres (4 ft) for females.[3] Other features can include an enlarged head and prominent forehead.[3] Complications can include sleep apnea or recurrent ear infections.[3] Achondroplasia includes the extremely rare short-limb skeletal dysplasia with severe combined immunodeficiency.
| Achondroplasia | |
|---|---|
 | |
| Jason "Wee Man" Acuña, an American actor and stunt performer with achondroplasia | |
| Pronunciation | |
| Specialty | Medical genetics |
| Symptoms | Short arms and legs, enlarged head, prominent forehead[3] |
| Complications | Ear infections, hyperlordosis, back pain, spinal stenosis, hydrocephalus[3] |
| Causes | Genetic (autosomal dominant mutation in the FGFR3 gene)[3] |
| Risk factors | Paternal age[4][3] |
| Diagnostic method | Based on symptoms, genetic testing if uncertain[5] |
| Differential diagnosis | Hypochondroplasia, thanatophoric dysplasia, cartilage-hair hypoplasia, pseudoachondroplasia[5] |
| Treatment | Support groups, growth hormone therapy, treatment of complications[5] |
| Frequency | 1 in 27,500 people[3] |
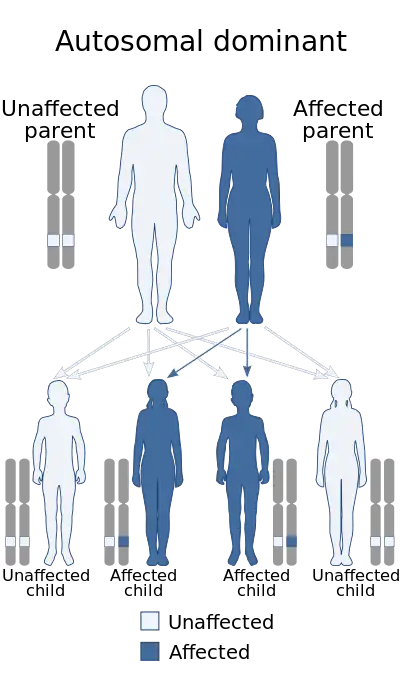
Achondroplasia is caused by a mutation in the fibroblast growth factor receptor 3 (FGFR3) gene that results in its protein being overactive.[3] Achondroplasia results in impaired endochondral bone growth (bone growth within cartilage).[6] The disorder has an autosomal dominant mode of inheritance, meaning only one mutated copy of the gene is required for the condition to occur.[7] About 80% of cases occur in children of parents without the disease, and result from a new (de novo, or sporadic) mutation, which most commonly originates as a spontaneous change during spermatogenesis.[5] The rest are inherited from a parent with the condition.[3] The risk of a new mutation increases with the age of the father.[4] In families with two affected parents, children who inherit both affected genes typically die before birth or in early infancy from breathing difficulties.[3] The condition is generally diagnosed based on the clinical features but may be confirmed by genetic testing.[5]
Treatments may include support groups and growth hormone therapy.[5] Efforts to treat or prevent complications such as obesity, hydrocephalus, obstructive sleep apnea, middle ear infections or spinal stenosis may be required.[5] Achondroplasia is the most common cause of dwarfism[4] and affects about 1 in 27,500 people.[3]
Signs and symptoms
- Disproportionate dwarfism
- Shortening of the proximal limbs (called rhizomelic shortening)
- Short fingers and toes, with "trident hands" (short hands with stubby fingers, and a separation between the middle and ring fingers – reminiscent of a trident on fetal ultrasound [8])
- Large head with prominent forehead frontal bossing
- Small midface with a flattened nasal bridge
- Spinal kyphosis (convex curvature) or lordosis (concave curvature)
- Varus (bowleg) or valgus (knock knee) deformities
- Frequent ear infections (due to Eustachian tube blockages), sleep apnea (which can be central or obstructive), and hydrocephalus
Children
Children with achondroplasia often have less muscle tone; because of this it is common for them to have delayed walking and motor skills. It is also common for children to have bowed legs, scoliosis, lordosis, arthritis, issues with joint flexibility, breathing problems, ear infections, and crowded teeth.[9] These issues can be treated with surgery, braces, or physical therapy.
Hydrocephalus is a severe effect associated with achondroplasia in children. This condition occurs when cerebrospinal fluid is not able to flow in and out of the skull because of how the spine narrows.[10] This fluid build up is associated with an enlarged head, vomiting, lethargy, headaches, and irritability.[11] A shunt surgery is commonly performed to treat this condition, but an endoscopic third ventriculostomy can also be done.[12]
Adults
Adults with achondroplasia often face issues with obesity and sleep apnea. It is also typical for adults to experience numbness or tingling in their legs because of nerve compression.
Some research has found that adults with achondroplasia may also experience psychosocial complications, usually associated with short stature.[13][14]
Pregnancy in women with achondroplasia is considered higher risk. Women with achondroplasia generally have their babies delivered through C-sections to prevent complications that could occur with a natural birth.[15] The life expectancy of people with achondroplasia is approximately 10 years less than average.[5]
Causes
Achondroplasia is caused by a mutation in fibroblast growth factor receptor 3 (FGFR3) gene.[16] This gene encodes a protein called fibroblast growth factor receptor 3, which contributes to the production of collagen and other structural components in tissues and bones.[17] When the FGFR3 gene is mutated it interferes with how this protein interacts with growth factors leading to complications with bone production. Cartilage is not able to fully develop into bone, causing the individual to be disproportionately shorter in height. [18]
In normal development, FGFR3 has a negative regulatory effect on bone growth. In achondroplasia, the mutated form of the receptor is constitutively active, and this leads to severely shortened bones. This is an example of a gain of function mutation. The effect is genetically dominant, with one variant of the FGFR3 gene being sufficient to cause achondroplasia, while two copies of the mutant gene are invariably fatal (recessive lethal) before or shortly after birth. This occurs due to respiratory failure from an underdeveloped ribcage.[3] People with achondroplasia are often born to parents that do not have the condition due to spontaneous mutation.[19]
Where achondroplasia is inherited, its pattern is autosomal dominant. In couples where one partner has achondroplasia there is a 50% chance of passing the disorder on to their child every pregnancy. In situations where both parents have achondroplasia there is a 50% chance the child will have achondroplasia, 25% chance the child will not, and a 25% chance that the child will inherit the gene from both parents resulting in double dominance and leading to lethal bone dysplasia.[20]
Studies have demonstrated that new gene mutations for achondroplasia are exclusively inherited from the father and occur during spermatogenesis; it has been theorized that sperm carrying the mutation in FGFR3 have a selective advantage over sperm with normal FGFR3.[4] The frequency of mutations in sperm leading to achondroplasia increases in proportion to paternal age, as well as in proportion to exposure to ionizing radiation.[21] The occurrence rate of achondroplasia in the children of fathers over 50 years of age is 1 in 1,875, compared to 1 in 15,000 in the general population.[22] Research by urologist Harry Fisch of the Male Reproductive Center at Columbia Presbyterian Hospital in 2013 indicated that in humans this defect may be exclusively inherited from the father and becomes increasingly probable with paternal age, specifically males reproducing after 35.[23]
There are two other syndromes with a genetic basis similar to achondroplasia: hypochondroplasia and thanatophoric dysplasia.
Diagnosis

Achondroplasia can be detected before birth by prenatal ultrasound, although signs are often subtle and not apparent before the 24th week of pregnancy.[24] A DNA test can be performed before birth to detect homozygosity, wherein two copies of the mutant gene are inherited, a lethal condition leading to stillbirths. Postnatal diagnosis of achondroplasia is typically uncomplicated, involving an assessment of physical and radiographic features.[25] Clinical features include megalocephaly, short limbs, prominent forehead, thoracolumbar kyphosis and mid-face hypoplasia.[26] Complications like dental malocclusion, hydrocephalus and repeated otitis media can be observed.[26] The risk of death in infancy is increased due to the likelihood of compression of the spinal cord with or without upper airway obstruction.
Radiologic findings
A skeletal survey is useful to confirm the diagnosis of achondroplasia. The skull is large, with a narrow foramen magnum, and relatively small skull base. The vertebral bodies are short and flattened with relatively large intervertebral disk height, and there is congenitally narrowed spinal canal. The iliac wings are small and squared, with a narrow sciatic notch and horizontal acetabular roof.[27][28] The tubular bones are short and thick with metaphyseal cupping and flaring and irregular growth plates.[27] Fibular overgrowth is present. The hand is broad with short metacarpals and phalanges, and a trident configuration. The ribs are short with cupped anterior ends.[27] If the radiographic features are not classic, a search for a different diagnosis should be entertained. Because of the extremely deformed bone structure, people with achondroplasia are often "double jointed". The diagnosis can be made by fetal ultrasound by progressive discordance between the short femur length and biparietal diameter by age. The trident hand configuration can be seen if the fingers are fully extended.
Another common characteristic of the syndrome is thoracolumbar gibbus in infancy.[29]
Treatment
There is no known cure for achondroplasia even though the cause of the mutation in the growth factor receptor has been found. Although used by those without achondroplasia to aid in growth, human growth hormone does not help people with achondroplasia, which involve a different hormonal pathway. Usually, the best results appear within the first and second year of therapy.[30] After the second year of growth hormone therapy, beneficial bone growth decreases,[31] so the therapy is not a satisfactory long-term treatment.[30] As of December 2020, the treatment of achondroplasia with human growth hormone was approved only in Japan.[32]
An experimental drug called vosoritide has shown promise in stage 3 human trials, although its long-term effects are unknown.[33]
Limb-lengthening will increase the length of the legs and arms of someone with achondroplasia,[34] but little medical consensus exists regarding this practice. The age of surgery can vary from early childhood to adulthood.[35]
Research has also shown that introducing parents of children with achondroplasia to support and advocacy groups at the time of diagnosis can improve outcomes.[36] Several patient advocacy groups exist to support people with achondroplasia and their families.[37]
In October 2023, the FDA approved and expanded the use of vosoritide, a once-daily injection for the treatment of children under the age of 5 with achondroplasia. It had previously been approved in 2021 for treating the genetic disorder in children aged five and older under the FDA's accelerated approval pathway.[38]
Epidemiology
Achondroplasia is one of several congenital conditions with similar presentations, such as osteogenesis imperfecta, multiple epiphyseal dysplasia tarda, achondrogenesis, osteopetrosis, and thanatophoric dysplasia. This makes estimates of prevalence difficult, with changing and subjective diagnostic criteria over time. One detailed and long-running study in the Netherlands found that the prevalence determined at birth was only 1.3 per 100,000 live births.[39] Another study at the same time found a rate of 1 per 10,000.[39] A 2020 review and meta-analysis estimated a worldwide prevalence of 4.6 per 100,000.[40]
Research
As of 2019, tentative evidence has found that the experimental peptide drug vosoritide increases growth velocity in those with achondroplasia. The drug inhibits the activity of FGFR3.[41]
Psychological and social aspects
In addition to physical challenges, individuals with achondroplasia may also experience psychological challenges such as fear or negative perception of individuals with achondroplasia. Gollust et al have indicated that adults with achondroplasia tend to have lower self-esteem, annual income, educational attainment, and overall quality of life (QOL) when compared to their unaffected siblings.[42] Interestingly, the Golust study revealed that the subjects were as likely to cite disadvantages relating to social barriers as those relating to health issues and functioning.
On the other hand, other investigators, such as Ancona, state that for many individuals in immediate environments that have natural acceptance of the condition from the beginning, their main challenge lies in adapting to a world designed for those without the condition. However, when society rejects the condition from the start and associates it with destructive anxiety, it significantly damages the individual's self-image and leads to their social exclusion. Thus, the author hypothesizes, an accepting environment is crucial to prevent significant suffering for individuals with achondroplasia and to ensure the best outcomes for corrective interventions, rather than perpetuating rejection. [43]
Similarly, a study conducted in Japan by Nishimura and Hanaki found that children with achondroplasia faced challenges related to their short stature, but there was no indication of psychosocial maladjustment. They hypothesized that focusing on coping strategies and self-efficacy may play a crucial role in promoting psychological well-being among children with achondroplasia.[44]
Social support and peer connections can be important for individuals with achondroplasia. Support groups, online communities, and advocacy organizations can provide a sense of belonging and can help individuals with achondroplasia connect with others who understand their experiences. Additionally, these communities can serve as a resource for information and support for both individuals with achondroplasia and their families. In the United States, The Little People of America (LPA) is a national organization that provides support, resources, and advocacy for individuals with dwarfism, including achondroplasia.[45]
Animals

Based on their disproportionate dwarfism, some dog breeds traditionally have been classified as "achondroplastic". This is the case for the dachshund, basset hound, corgi and bulldog breeds.[46][47][48] Data from whole genome association studies in short-limbed dogs reveal a strong association of this trait with a retro-gene coding for fibroblast growth factor 4 (FGF4).[49] Therefore, it seems unlikely that dogs and humans are achondroplastic for the same reasons. However, histological studies in some achondroplastic dog breeds have shown altered cell patterns in cartilage that are very similar to those observed in humans exhibiting achondroplasia.[50]
A similar form of achondroplasia was found in a litter of piglets from a phenotypically normal Danish sow. The dwarfism was inherited dominant in the offspring from this litter. The piglets were born phenotypically normal but became more and more symptomatic as they reached maturity.[51] This involved a mutation of the protein collagen, type X, alpha 1, encoded by the COL10A1 gene. In humans a similar mutation (G595E) has been associated with Schmid metaphyseal chondrodysplasia (SMCD), a relatively mild skeletal disorder that is also associated with dwarfism.
The now extinct Ancon sheep was created by humans through the selective breeding of common domestic sheep with achondroplasia. The average-sized torso combined with the relatively smaller legs produced by achondroplasia was valued for making affected sheep less likely to escape without affecting the amount of wool or meat each sheep produced.[52]
See also
References
- "Achondroplasia". Lexico UK English Dictionary. Oxford University Press. Archived from the original on 11 December 2019.
- "Achondroplasia". Merriam-Webster.com Dictionary.
- "Achondroplasia". Genetics Home Reference. May 2012. Retrieved 12 December 2017.
- Horton, William A; Hall, Judith G; Hecht, Jacqueline T (July 2007). "Achondroplasia". The Lancet. 370 (9582): 162–172. doi:10.1016/S0140-6736(07)61090-3. PMID 17630040. S2CID 208788746.
- Pauli, RM; Adam, MP; Ardinger, HH; Pagon, RA; Wallace, SE; Bean, LJH; Mefford, HC; Stephens, K; Amemiya, A; Ledbetter, N (2012). "Achondroplasia". GeneReviews. PMID 20301331.
- Pauli, Richard M. (2019). "Achondroplasia: A comprehensive clinical review". Orphanet Journal of Rare Diseases. 14 (1): 1. doi:10.1186/s13023-018-0972-6. PMC 6318916. PMID 30606190.
- "Achondroplasia". Genetic and Rare Diseases Information Center (GARD) – an NCATS Program. 2016. Retrieved 12 December 2017.
- "Trident hand". Radiopaedia. Retrieved 31 May 2022.
- "Dwarfism". kidshealth.org. Retrieved 26 September 2018.
- "Achondroplasia | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program". rarediseases.info.nih.gov. Retrieved 26 September 2018.
- Kieffer, Sara. "Achondroplasia | Johns Hopkins Pediatric Neurosurgery". Retrieved 26 September 2018.
- "Hydrocephalus – Diagnosis and treatment – Mayo Clinic". www.mayoclinic.org. Retrieved 26 September 2018.
- Pauli, Richard M. (2019). "Achondroplasia: A comprehensive clinical review". Orphanet Journal of Rare Diseases. 14 (1): 1. doi:10.1186/s13023-018-0972-6. PMC 6318916. PMID 30606190.
- Constantinides, Constantinos; Landis, Sarah H.; Jarrett, James; Quinn, Jennifer; Ireland, Penelope J. (2021). "Quality of life, physical functioning, and psychosocial function among patients with achondroplasia: A targeted literature review". Disability and Rehabilitation. 44 (21): 6166–6178. doi:10.1080/09638288.2021.1963853. PMID 34403286. S2CID 237198129.
- Services, Department of Health & Human. "Dwarfism". Retrieved 26 September 2018.
- "Learning About Achondroplasia". National Human Genome Research Institute (NHGRI). Retrieved 26 September 2018.
- Reference, Genetics Home. "FGFR3 gene". Genetics Home Reference. Retrieved 26 September 2018.
- Horton, William A; Hall, Judith G; Hecht, Jacqueline T (July 2007). "Achondroplasia". The Lancet. 370 (9582): 162–172. doi:10.1016/s0140-6736(07)61090-3. ISSN 0140-6736. PMID 17630040. S2CID 208788746.
- Richette P, Bardin T, Stheneur C (2007). "Achondroplasia: From genotype to phenotype". Joint Bone Spine. 75 (2): 125–30. doi:10.1016/j.jbspin.2007.06.007. PMID 17950653.
- "Achondroplasia". Retrieved 26 September 2018.
- Wyrobek AJ, Eskenazi B, Young S, Arnheim N, Tiemann-Boege I, Jabs EW, Glaser RL, Pearson FS, Evenson D (2006). "Advancing age has differential effects on DNA damage, chromatin integrity, gene mutations, and aneuploidies in sperm". Proceedings of the National Academy of Sciences of the United States of America. 103 (25): 9601–9606. Bibcode:2006PNAS..103.9601W. doi:10.1073/pnas.0506468103. PMC 1480453. PMID 16766665.
- Kovac, Jason R; Addai, Josephine; Smith, Ryan P; Coward, Robert M; Lamb, Dolores J; Lipshultz, Larry I (November 2013). "The effects of advanced paternal age on fertility". Asian Journal of Andrology. 15 (6): 723–728. doi:10.1038/aja.2013.92. PMC 3854059. PMID 23912310.
- Harry Fisch (24 September 2013). The Male Biological Clock: The Startling News About Aging, Sexuality, and Fertility in Men. Simon and Schuster. pp. 11–. ISBN 978-1-4767-4082-9.
- Savarirayan, Ravi; et al. (2021). "International Consensus Statement on the diagnosis, multidisciplinary management and lifelong care of individuals with achondroplasia". Nature Reviews Endocrinology. 18 (3): 173–189. doi:10.1038/s41574-021-00595-x. PMID 34837063. S2CID 244638495.
Ultrasound findings of achondroplasia are generally not apparent until 24 weeks of gestation and are often quite subtle.
- Savarirayan, Ravi; et al. (2021). "International Consensus Statement on the diagnosis, multidisciplinary management and lifelong care of individuals with achondroplasia". Nature Reviews Endocrinology. 18 (3): 173–189. doi:10.1038/s41574-021-00595-x. PMID 34837063. S2CID 244638495.
The postnatal diagnosis of achondroplasia is fairly straightforward. A combination of key clinical (that is, macrocephaly, short limbed-short stature with rhizomelia and redundant skin folds) and radiographic (that is, characteristic pelvis with short and square ilia, narrow sacro-sciatic notches and narrowing interpedicular distances in the lumbar vertebral spine progressing from L1 to L5) features enables accurate diagnosis in most people with achondroplasia.
- Beattie, R.M.; Champion, M.P., eds. (2004). Essential questions in paediatrics for MRCPCH (1st ed.). Knutsford, Cheshire: PasTest. ISBN 978-1-901198-99-7.
- EL-Sobky, TA; Shawky, RM; Sakr, HM; Elsayed, SM; Elsayed, NS; Ragheb, SG; Gamal, R (15 November 2017). "A systematized approach to radiographic assessment of commonly seen genetic bone diseases in children: A pictorial review". J Musculoskelet Surg Res. 1 (2): 25. doi:10.4103/jmsr.jmsr_28_17. S2CID 79825711.
- "Achondroplasia Pelvis". Archived from the original on 22 October 2007. Retrieved 28 November 2007.
- Savarirayan, Ravi; et al. (2021). "International Consensus Statement on the diagnosis, multidisciplinary management and lifelong care of individuals with achondroplasia". Nature Reviews Endocrinology. 18 (3): 173–189. doi:10.1038/s41574-021-00595-x. PMID 34837063. S2CID 244638495.
Spinal thoracolumbar kyphosis (gibbus) in infants with achondroplasia is common but should resolve when the child begins to mobilize.
- Vajo, Zoltan; Francomano, Clair A.; Wilkin, Douglas J. (1 February 2000). "The Molecular and Genetic Basis of Fibroblast Growth Factor Receptor 3 Disorders: The Achondroplasia Family of Skeletal Dysplasias, Muenke Craniosynostosis, and Crouzon Syndrome with Acanthosis Nigricans". Endocrine Reviews. 21 (1): 23–39. doi:10.1210/edrv.21.1.0387. PMID 10696568.
- Aviezer, David; Golembo, Myriam; Yayon, Avner (30 June 2003). "Fibroblast Growth Factor Receptor-3 as a Therapeutic Target for Achondroplasia - Genetic Short Limbed Dwarfism". Current Drug Targets. 4 (5): 353–365. doi:10.2174/1389450033490993. PMID 12816345.
- Legeai-Mallet, Laurence; Savarirayan, Ravi (2020). "Novel therapeutic approaches for the treatment of achondroplasia". Bone. 141: 115579. doi:10.1016/j.bone.2020.115579. PMID 32795681. S2CID 221133224.
One therapy offered to ACH patients is treatment with recombinant human growth (r-hGH) (approved today only in Japan).
- Savarirayan, Ravi; Tofts, Louise; Irving, Melita; Wilcox, William; Bacino, Carlos A.; Hoover-Fong, Julie; Font, Rosendo Ullot; Harmatz, Paul; Rutsch, Frank; Bober, Michael B.; Polgreen, Lynda E.; Ginebreda, Ignacio; Mohnike, Klaus; Charrow, Joel; Hoernschemeyer, Daniel; Ozono, Keiichi; Alanay, Yasemin; Arundel, Paul; Kagami, Shoji; Yasui, Natsuo; White, Klane K.; Saal, Howard M.; Leiva-Gea, Antonio; Luna-González, Felipe; Mochizuki, Hiroshi; Basel, Donald; Porco, Dania M.; Jayaram, Kala; Fisheleva, Elena; Huntsman-Labed, Alice; Day, Jonathan (5 September 2020). "Once-daily, subcutaneous vosoritide therapy in children with achondroplasia: a randomised, double-blind, phase 3, placebo-controlled, multicentre trial". The Lancet. 396 (10252): 684–692. doi:10.1016/S0140-6736(20)31541-5. PMID 32891212. S2CID 221472752.
- Kitoh H, Kitakoji T, Tsuchiya H, Katoh M, Ishiguro N (2007). "Distraction osteogenesis of the lower extremity in patients that have achondroplasia/hypochondroplasia treated with transplantation of culture-expanded bone marrow cells and platelet-rich plasma". J Pediatr Orthop. 27 (6): 629–34. doi:10.1097/BPO.0b013e318093f523. PMID 17717461. S2CID 42226362.
- Savarirayan, Ravi; et al. (2021). "International Consensus Statement on the diagnosis, multidisciplinary management and lifelong care of individuals with achondroplasia". Nature Reviews Endocrinology. 18 (3): 173–189. doi:10.1038/s41574-021-00595-x. PMID 34837063. S2CID 244638495.
Although evidence in this area is scarce, limb lengthening is advised in some countries and not recommended in others. … The timing of limb lengthening varies and has been performed from early childhood to adult life in individuals with achondroplasia.
- Savarirayan, Ravi; et al. (2021). "International Consensus Statement on the diagnosis, multidisciplinary management and lifelong care of individuals with achondroplasia". Nature Reviews Endocrinology. 18 (3): 173–189. doi:10.1038/s41574-021-00595-x. PMID 34837063. S2CID 244638495.
Introducing parents to advocacy and support groups has been proven beneficial.
- "Associations". Beyond Achondroplasia. Retrieved 2 January 2022.
- Jain, Pratik (20 October 2023). "BioMarin's dwarfism therapy gets FDA nod for expanded use". Reuters. Retrieved 24 October 2023.
- Online Mendelian Inheritance in Man (OMIM): ACHONDROPLASIA; ACH - 100800
- Foreman, Pamela K.; Kessel, Femke; Hoorn, Rosa; Bosch, Judith; Shediac, Renée; Landis, Sarah (2020). "Birth prevalence of achondroplasia: A systematic literature review and meta‐analysis". American Journal of Medical Genetics Part A. 182 (10): 2297–2316. doi:10.1002/ajmg.a.61787. PMC 7540685. PMID 32803853.
- Savarirayan, Ravi (4 July 2019). "C-Type Natriuretic Peptide Analogue Therapy in Children with Achondroplasia". New England Journal of Medicine. 381 (1): 25–35. doi:10.1056/NEJMoa1813446. PMID 31269546.
- Gollust, Sarah E.; Thompson, Richard E.; Gooding, Holly C.; Biesecker, Barbara B. (2003). "Living with achondroplasia in an average-sized world: An assessment of quality of life". American Journal of Medical Genetics. 120A (4): 447–458. doi:10.1002/ajmg.a.20127. PMID 12884421. S2CID 38614817.
- Ancona, Leonardo (1988). "The Psychodynamics of Achondroplasia". Human Achondroplasia. pp. 447–451. doi:10.1007/978-1-4684-8712-1_56. ISBN 978-1-4684-8714-5. PMID 3240281.
{{cite book}}:|journal=ignored (help) - Nishimura, Naoko; Hanaki, Keiichi (2014). "Psychosocial profiles of children with achondroplasia in terms of their short stature-related stress: A nationwide survey in Japan". Journal of Clinical Nursing. 23 (21–22): 3045–3056. doi:10.1111/jocn.12531. PMID 25453127.
- Little People of America. (n.d.). About LPA. Retrieved from https://www.lpaonline.org/about-lpa
- "WebMD".
- Jones, T.C.; Hunt, R.D. (1979). "The musculoskeletal system". In Jones, T.C.; Hunt, R.D.; Smith, H.A. (eds.). Veterinary Pathology (5th ed.). Philadelphia: Lea & Febiger. pp. 1175–6. ISBN 978-0812107890.
- Willis M.B. (1989). "Inheritance of specific skeletal and structural defects". In Willis M.B. (ed.). Genetics of the Dog. Great Britain: Howell Book House. pp. 119–120. ISBN 978-0876055519.
- Parker HG, VonHoldt BM, Quignon P, et al. (August 2009). "An expressed fgf4 retrogene is associated with breed-defining chondrodysplasia in domestic dogs". Science. 325 (5943): 995–8. Bibcode:2009Sci...325..995P. doi:10.1126/science.1173275. PMC 2748762. PMID 19608863.
- Braund KG, Ghosh P, Taylor TK, Larsen LH (September 1975). "Morphological studies of the canine intervertebral disc. The assignment of the beagle to the achondroplastic classification". Res. Vet. Sci. 19 (2): 167–72. doi:10.1016/S0034-5288(18)33527-6. PMID 1166121.
- Nielsen VH, Bendixen C, Arnbjerg J, et al. (December 2000). "Abnormal growth plate function in pigs carrying a dominant mutation in type X collagen". Mamm. Genome. 11 (12): 1087–92. doi:10.1007/s003350010212. PMID 11130976. S2CID 2786778.
- Gidney, Louisa (May–June 1019). "Earliest Archaeological Evidence of the Ancon Mutation in Sheep from Leicester, UK". International Journal of Osteoarchaeology. 15 (27): 318–321. doi:10.1002/oa.872. ISSN 1099-1212.
External links
- Achondroplasia at Curlie
- Pauli RM (1998). "Achondroplasia". In Pagon RA, Bird TD, Dolan CR, et al. (eds.). GeneReviews. Seattle WA: University of Washington, Seattle. PMID 20301331. NBK1152.